In an unexpected announcement pre-July 4th the big news was Obamacare Employer Mandate Delayed with penalties under the Affordable Care Act (ACA) until 2015. The mandate also known as the “Employer Shared Responsibility” requires employers with 50 or more FTEs to offer affordable health insurance coverage to their workers or face financial penalties for not doing so. Those penalties would originally have been applied beginning in 2014.
There has been a follow up guidance issued last week July 9th by the IRS. According to the IRS, the delay will give employers more time to prepare for the change in how health insurance is provided and will also give the Obama Administration time to simplify the insurance-related reporting requirements that employers face. This transition relief appears to come with “no strings attached.” Although the IRS guidance encourages employers to voluntarily comply with the employer mandate and maintain or expand health care coverage in 2014, the IRS will not impose penalties for a failure to do so.
Although the IRS guidance encourages employers to voluntarily comply with the employer mandate and maintain or expand health care coverage in 2014, the IRS will not impose penalties for a failure to do so.Notably, the guidance issued on July 9th also does not require employers to make “good faith” efforts to comply. As a result of this transition year, employers will have the option of deciding to what extent (if any) they will continue efforts to comply with the employer mandate during 2014.
Employers who intended to rely on one of the transition rules previously announced for 2014 should keep in mind that the latest IRS guidance does not provide special transition rules for 2015. Other group health plan requuirements still apply as discussed in our prior blog Essential Health Benefits Not Delayed.
This means that for plan years beginning on and after January 1, 2014, all group health plans must:
Eliminate all pre-existing condition exclusions (regardless of age);
Maximum Cost Sharing Deductible to $2,000/individual ($4,000/family); limit in-network out-of-pocket maximums to $6,350/individual ($12,700/family)
Individual Mandate Still Applies. individuals will still be required to obtain health care coverage or pay a penalty for each month they do not have coverage, beginning January 1, 2014
Exchanges (Marketplaces) Open for Enrollment October 1, 2013.
The IRS notice makes it clear that individuals who enroll in coverage on the marketplaces will continue to be eligible for a premium tax credit if their household income is within a specified range and they are not eligible for other minimum essential coverage.
Employers Must Send Notice of Exchanges (Marketplaces) Before October 1, 2013. These notices must be sent to current employees by October 1, 2013. Then, beginning October 1, 2013, employers must send this notice to new hires within 14 days of their start date.
New taxes still apply – Patient Centered Outcomes Research Institute (PCORI) excise taxes and transitional reinsurance program fees;HRA/HSA/FSA clients also pay a monthly $1/employee tax.
We will continue to monitor ACA developments and will provide you relevant updated information when available. In the meantime, please visit to view past blogs and Legislative Alerts at https://360peo.com/feed.
Obama administration announced that the employer shared responsibility mandate also known as “Pay or Play” aspect of the Patient Protection and Affordable Care Act (PPACA) will be delayed by one year.
This mandate requires businesses with 50 or more workers to provide health insurance coverage to employees. As a result, the administration will start enforcing the mandate in 2015, rather than January 1, 2014, in an effort to give businesses more time to prepare.
There will be additional changes tied to this delay, and the administration has stated that they will provide formal guidance within the next week.
More details will be available for our July 11th WebMeeting. Medical Solutions Corp is working with the various regulatory agencies to understand the specifics surrounding this ruling, and will continue to provide updates through Legislative Alerts and on our blog.
Final Wellness Incentive Rule Released. Final rules set forth the criteria for wellness programsoffered in connection with group health plans that must be satisfied in order for the plan to qualify for an exception to the prohibition on discrimination based on health status under the federal Health Insurance Portability and Accountability Act (HIPAA). The final rules will be effective for plan years beginning on or after January 1, 2014.
Many employers already offered incentives for employees participating in wellness programs. The main change in the new rule is an increase in the maximum incentive levels for several PPACA designated programs. For smoking cessation efforts, employers will be allowed to offer a reward or penalty of up to 50% of an employee’s health plan cost. For all other wellness programs, the number will be 30%, up from the current 20%. These increases are intended to promote healthy behavior which in turn, advocates claim, reduce health care spending.
Key Highlights Significant provisions included in the final rules include:
Increasing the maximum permissible reward under a health-contingent wellness program, from 20% to 30% of the cost of coverage;
Further increasing the maximum permissible reward for wellness programs designed to prevent or reduce tobacco use, from 20% to 50% of the cost of coverage; and
Clarifications regarding the reasonable design of health-contingent wellness programs and the reasonable alternatives they must offer in order to avoid prohibited discrimination.
Types of Participatory Wellness Programs The final rules continue to divide wellness programs into two categories:
1)”participatory wellness programs,” which are a majority of wellness programs,
2)and “health-contingent wellness programs.”
A participatory wellness program is one that either does not provide a reward or does not include any conditions for obtaining a reward that are based on an individual satisfying a standard related to a health factor. These include programs that reimburse for the cost of membership in a fitness center; provide a reward to employees for attending a monthly, no-cost health education seminar; or reward employees who complete a health risk assessment, without requiring them to take further action.
Participatory wellness programs are generally permissible under the HIPAA nondiscrimination rules, provided they are available to all similarly situated individuals regardless of health status.
Health-Contingent Wellness Programs In contrast, a health-contingent wellness program requires an individual to satisfy a standard related to a health factor to obtain a reward. This standard may be performing or completing an activity (an “activity-only wellness program”), or it may be attaining or maintaining a specific health outcome (an “outcome-based wellness program”).
Examples of health-contingent wellness programs include programs that provide a reward to those who do not use, or decrease their use of, tobacco, or programs that reward those who achieve a specified health-related goal, such as a specified cholesterol level, weight, or body mass index, as well as those who fail to meet such goals but take certain other healthy actions.
In order to qualify for an exception to the HIPAA nondiscrimination rules, health-contingent wellness programs must meet five additional standards related to frequency of opportunity to qualify; size of the reward; reasonable design; uniform availability and reasonable alternative standards; and notice of the availability of reasonable alternative standards.
Example
The final rule provides an example of how this reward/penalty might work:
An employer sponsors a group health plan. The annual premium for employee-only coverage is $6,000 (of which the employer pays $4,500 per year and the employee pays $1,500 per year). The plan offers employees a health-contingent wellness program with several components, focused on exercise, blood sugar, weight, cholesterol, and blood pressure. The reward for compliance is an annual premium rebate of $600…[T]he plan also imposes an additional $2,000 tobacco premium surcharge on employees who have used tobacco in the last 12 months and who have not enrolled in the plan’s tobacco cessation program (Those who participate…are not assessed the $2,000 surcharge).
The total of all the rewards (including the absence of a surcharge for participating in the tobacco program) is $2,600…which does not exceed the applicable percentage of 50% of the total annual cost of employee-only coverage ($6,000 x 50%=$3,000). Tested separately, the $600 reward for the wellness program [excluding] tobacco use does not exceed the applicable percentage of 30 percent of the total annual cost of employee-only coverage ($6,000 x 30%=$1,800).
In excellent article in the Atlantic –The Future of Getting Paid to Be Healthy“Incentive programs are not wellness programs,” said Dr. Ronald Goetzel, Director of Emory University’s Institute for Health and Productivity Research and President and CEO of The Health Project. “That can be a component, when done smartly, of a comprehensive program, but if that’s all your program is going to be, you’re going to fail miserably, and people are going to be resentful,” he explained. According to Goetzel — who has studied worksite wellness programs at large corporations such as Dow Chemical and Johnson & Johnson, and is being funded by the Centers for Disease Control and Prevention to study best practices in the field — incentive programs can help get people excited about health and keep them on track, but ultimately people’s habits will only change if they are given the resources to change them and if the workplace norms and environments change.
Without the other pieces to facilitate behavior change — healthy cafeterias, opportunities to exercise, flexible work hours, supportive leadership and middle managers, and health risk assessments and coaching — incentive programs will only penalize, not change, those who are least healthy.
For more information, you may review the final rules in their entirety. For MMS Corp previous blogs on wellness, click here. we will keep you posted on future PPACA wellness program opportunities. In the meantime, please visit to view past blogs and Legislative Alerts at https://360peo.com/feed.
The views expressed in this post do not necessarily reflect the official policy, position, or opinions of MMS Corp. This update is provided for informational purposes. Please consult with a licensed accountant or attorney regarding any legal and tax matters discussed herein.
Fiscal Cliff Deal: Doc Cuts Spared. Happy 2013 Fiscal Cliff averted! At least for another year the dreaded 27% Medicare reimbursement have been spared. The so-called “doc fix” would boost the deficit by $31 billion. The President stood firm against any proposed Republican cuts to the Affordable Care Act.
The fear in provider cuts is grounded. According to The Lewin Report Patient Protection and Affordable Care Act (PPACA): Long Term Costs for Governments, Employers, Families and Providers “About half of program costs will be funded with reductions in payments to providers and health plans under the Medicare and Medicaid programs, which the CBO estimates will amount to $498 billion over the ten year period“. The new cost estimate has been updated to $1.4445 trillion from original estimate $938 billion over 10 years.
With millions of new uninsured patients slated to enter the system this would help providers recover reimbursement losses. Additionally, the President was firmly against any Provider cuts in 2013.
The Lewin Report predicts in fact that Provider Reimbursement will recover losses long term and in fact increase gross payments to $129.8 billion under the Act.
“..estimate that utilization of physician services will increase by about $102.7 billion under the Act. This estimate reflects Medicaid the payment levels for the portion of newly insured people covered under that program and commercial payment levels for those who become covered under private insurance. As discussed above, our key assumption is that utilization of services for newly insured people adjusts to the levels reported by insured individuals with similar age, gender, health status and income characteristics. Physicians also will be paid for services formerly provided free to uninsured people resulting in revenues of $8.4 billion. There will be an increase in reimbursement for people who shift from Medicaid to private coverage, and payment rates for Medicare primary care services will be increased for a three year period under the Act. These factors will add 18.7 billion in revenues for physicians.
While there was large Senate consensus 89-8 approval for the American Taxpayer Relief Act the health care debate is far from over. With rising health care costs, combined with the aging of the baby boomers, means the entitlement programs will remain at the heart of the tax-and-spending battles to come.
New Proposed Rules for Wellness ProgramsIn another step forward to ncentivize wellness new proposal can give discounts for managing good health much like good drivers with auto insurance.Newproposed rules issued under Health Care Reform address certain amendments to the nondiscrimination requirements for group health plans offering a wellness program to comply with the federal Health Insurance Portability and Accountability Act(HIPAA).Specifically, the proposed rules would increase the maximum permissible reward under a wellness program that requires an individual to satisfy a standard based on a health factor in order to obtain a reward, from 20% to 30% of the cost of coverage (and to 50% for programs designed to prevent or reduce tobacco use). The rules also include other proposed clarifications regarding the requirements for such wellness programs to avoid prohibited discrimination, including reasonable design and reasonable alternatives that must be offered for individuals to obtain the reward.Other Proposed Rules Released Under Health Care Reform Separately, new proposed rules have been issued for health insurance companies regarding the law’s requirements related to guaranteed availability of coverage and essential health benefits.
Under one set of proposed rules, issuers offering non-grandfathered health insurance coverage in the individual or group market would be required to accept every individual and employer that applies for coverage, with limited exceptions. Issuers in the individual and small group markets would be allowed to vary premiums within limits, only based on age, tobacco use, family size, and geography.
Another set of proposed rules outline issuer standards related to coverage of “essential health benefits.” Essential health benefits are a core set of items and services that must be covered by non-grandfathered plans in the individual and small group markets beginning in 2014.
While its always been known a healthy livingfor employees makes a productive employee. Large businesses have benefited from a healthy work force as they can better afford programs and have a direct rate reduction in rates.
Although employers continue to use cost shifting to control health insurance expenses, many companies are also making wellness programs part of the overall strategy to keep costs down by keeping staff members healthy.“Our entire health care system is organized around treating diseases after they occur, not preventing them before they occur. We need a paradigm shift that places prevention at the center of our health priorities.” – Lynn C. Swann, Chairman, President’s Council on Physical Fitness and Sports
The new proposed rules would apply for plan years beginning on or after January 1, 2014. An overview of the proposed rules is available on Healthcare.gov. Our Summary by Year offers updates on other requirements related to Health Care Reform.
To no one’s surprise the InterfaithHospital in Brooklyn Files for Bankruptcy Protection– Dec3, 2012 NYT . In addition to the $130 Million in debt “…hospital estimates its cash spending will exceed its cash receipts by nearly $2 million, and it will have $7 million in unpaid obligations and $26 million in unpaid receivables, other than professional fees.”
The long time beleaguered hospital has been a stepchild of the State with multiple bail outs in the past decades. “Interfaith officials have said that they need $20 million from the state just to continue operating during the bankruptcy reorganization, and otherwise face the possibility that the hospital will close.” The State promised some financial support last year to accomplish an integrating Wyckoff Hospital, Brooklyn Hospital andInterfaith Hospitalby a Cuomo Pane Administration. Interfaith Hospital, located in Bedford Stuyvesant, took extreme steps to save cash by foregoing malpractice insurance – NYT “Troubled NY Hospital Forgo Coverage for Malpractice”.
Since health care is viewed as a right, the government has been subsidizing and encouraging its growth for decades, helping it to evolve into the juggernaut of 17% of the GNP that it is. Now, as Margaret Thatcher so famously said of all socialist experiments, “they have run out of other peoples’ money”. The law and the courts compel them to give everyone 21st century technology which costs more than many patients make in their whole life ! Now the medical industry is up against the limits of what they can pry out of the taxpayer and the private citizens but they are still compelled to offer insanely expensive health care to everyone. Very bright people try to wiggle around this dynamic but they are finding that they cant. We need to strike at the source, and accept : Health care is not a right, you don’t get it because you exist, you have to buy it. Only by accepting this truth can we begin to save a reasonable health care industry.
Unlike St Vincent’s Hospital Bankruptcy Closurein 2010 was a complete shock to NYC Health Community. For more than 150 years the hospital was a mainstay of Downtown Manhattan. It remains to be seen if this Administration will step in and save Interfaith Hospital again.
What is an Exchange? One of the centerpieces of the recently passed Patient Protection and Affordable Care Act
(PPACA) is the establishment of state based health insurance exchanges by the year 2014.
An “Exchange” is a mechanism for organizing the health insurance marketplace to help consumers and small businesses shop for coverage in a way that permits easy comparison of available plan options based on price, benefits, service and quality. By pooling individuals and small groups together, transaction costs can be reduced and transparency can be increased. Exchanges can create more efficient and competitive markets for individuals and small employers.
Historically, the individual and small group health insurance markets have suffered from adverse selection and high administrative costs, resulting in low value for consumers. “Exchanges” will allow individuals and small businesses to benefit from the pooling of risk, market leverage, and economies of scale that large businesses currently enjoy.
Beginning with an open enrollment period in 2013, Insurance agents and Benefits professionals will help individuals and small employers shop, select, and enroll in high-quality, affordable private health plans in these “Exchanges” to fit their specific needs at competitive prices. Individuals in these “Exchanges” may also be eligible to receive premium subsidies through the Federal or State government. By providing one-stop shopping, we will make purchasing health insurance easier and more understandable through these “Exchanges” and provide the same level of service that you have become accustomed to.
Middle-class people will be able to pick from a range of private insurance plans, and most people will be eligible for help from the government to pay their premiums.
Low-income people will be steered to safety-net programs for which they might qualify. This could be a problem in states that choose not to expand their Medicaid programs under a separate part of the health care law. In that case, many low-income residents in those states would remain uninsured.
Q: How will I know if I can get help with my health insurance premiums?
A: You’ll disclose your income to the exchange at the time you apply for coverage and they’ll let you know. Only legal residents of the United States can get financial assistance.
The health care law offers sliding-scale subsidies based on income for individuals and families making up to four times the federal poverty level, about $44,700 for singles, $92,200 for a family of four.
But do yourself a favor and read the fine print because the government’s help gets skimpier as household income increases.
For example, a family of four headed by a 40-year-old making $35,000 will get a $10,742 tax credit toward an annual premium of $12,130. They’d have to pay $1,388, about 4 percent of their income, or about $115 a month.
A similar hypothetical family making $90,000 will get a much smaller tax credit, $3,580, meaning they’d have to pay $8,550 of the same $12,130 policy. That works out to more than 9 percent of their income, or about $710 a month.
The estimates were made using the nonpartisan Kaiser Family Foundation’s online calculator. Some people will also be eligible for help with their copayments.
Final note: Though it’s called a “tax credit” the government assistance goes directly to the insurer. You won’t see a check.
Q: What will the benefits look like?
A: The coverage will be more comprehensive than what’s now typically available in the individual health insurance market, dominated by bare-bones plans. It will be more like what an established, successful small business offers its employees. Premiums are likely to be higher for some people, but government assistance should mostly compensate for that.
All plans in the exchange will have to cover a standard set of “essential health benefits,” including hospitalization, doctor visits, prescriptions, emergency room treatment, maternal and newborn care, and prevention. Insurers cannot turn away the sick or charge them more. Middle-aged and older adults can’t be charged more than three times what young people pay. Insurers can impose penalties on smokers.
Because the benefits will be similar, the biggest difference among plans will be something called “actuarial value.” A new term for consumers, it’s the share of expected health care costs that the plan will cover.
There will be four levels of coverage, from “bronze,” which will cover 60 percent of expected costs, to “platinum,” which will cover 90 percent. “Silver” and “gold” are in between. Bronze plans will charge the lowest premiums, but they’ll have the highest annual deductibles. Platinum plans will have the highest premiums and the lowest out-of-pocket cost sharing.
This part is insurance nerdy but an important point – The government’s subsidy will be tied to the premium for the second-lowest-cost plan at the silver coverage level that’s available in your area. You could take it and buy a lower cost bronze plan, saving money on premiums. But you’d have to be prepared for the higher annual deductible and copayments.
If you have additional questions regarding how SHOP Exchanges and Individual Exchanges can benefit you please contact our team at Millennium Medical Solutions Corp. Stay tuned for updates as more information gets released. We’re inside of 75 days until exchanges open, and information will be coming quickly in the next few months. Sign up for latest news updates.
There’s good news for patients visiting their doctors for preventive care – and for employers who want to keep their employees healthier. All non-grandfathered health plans now will cover the preventive health care without copays, deductibles or out-of-pocket fees.
Preventive care defined According to the law, preventive care includes “proven” preventive services that are rated A or B by the following agencies:
U.S. Preventive Services Task Force
Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention
Preventive care at Priority Health Priority Health’s Preventive Health Care Guidelines are prepared by Priority Health’s clinicians and outside consultants to help members in understanding exactly what services are covered for them, based on their age and sex. Our Preventive Health Care Guidelines are updated to include all of the services required by the Affordable Care Act.
Update: Effective August 1, 2012, services will be added to Priority Health’s Preventive Health Care Guidelines to incorporate the changes affecting women’s health announced in August 2011. New supplies such as contraceptives and breast pumps will be covered with no cost-sharing by members upon renewal of their employer’s non-grandfathered health plan after August 1, 2012.
Effective Preventive services must be included with no cost-sharing in all non-grandfathered plans. Preventive services may be covered by grandfathered plans subject to the member’s copay amount.
Regionaly For NY Metro, New England and Mid Atlantic this is one of these areas where health care reform simply requires what has always practiced: Cover preventive care services with minimal cost sharing. The deductible has never applied. Insurers have covered preventive at 100% on our HSA plans (Health Savings Accounts) since 2004. Example: Oxford Preventive Health Guidelines Member Flyer
Health plans must offer coverage to dependents on their parents’ plan(s) until the young adult turns 26. Coverage must offer the same benefits as for other dependents and can’t cost any more.
Dependent defined Eligible dependents:
Must be a dependent of the employee (son, daughter, stepson, or stepdaughter, legally adopted or eligible foster child*). Don’t have to be living with a parent
Don’t have to be living with a parent
Don’t have to be a dependent on their parents’ tax return
Don’t have to be full-time students
May be married (but plan doesn’t have to cover the dependent’s spouse or children)
Effective This applies to all health plans, including grandfathered plans. Grandfathered plans are not required to cover a dependent child if the dependent child is eligible for coverage under the dependent child’s own employer health plan until Jan. 1, 2014. Beginning in 2014, dependent children must be offered coverage whether or not they’re eligible for coverage under their employer’s plan.
Important notice about HSAs and dependents under age 26 While the Affordable Care Act allows parents to add their dependent children (up to age 26) to their health plans, the IRS has not changed its definition of a dependent for health savings accounts. This means that a person could have their 24-year-old child covered on their HSA-qualified high-deductible health plan, but not be eligible to use their HSA funds to pay for medical bills for that 24-year-old.
The IRS definition of a dependent is used when determining a dependent for HSA purposes. The account holder must be able to “claim” the child/relative as a dependent on their tax return. If the account holder can’t claim the child/relative as a dependent, then they can’t spend HSA dollars on services provided to that child/relative.
Here is a quick reminder of the IRS definition of a dependent:
Qualifying child:
Daughter, son, stepchild, sibling or stepsibling (or any descendant of these)
Has same principal place of abode for more than one-half of taxable year
Has not provided over ½ of own support during taxable year
AND not yet age 19 (not yet age 24 if student) at the end of the tax year
OR permanently and totally disabled
Qualifying relative:
Bears a relationship: daughter, son, stepchild, sibling or stepsibling (or any descendant of these), father, mother or ancestor, aunt, uncle, in-laws or an individual who has his/her principal place of residence the home of account owner
Receives more than half of support from account owner
Companies in the Salt Lake City area know productivity is higher and health costs are lower when employees have ways to exercise and reduce stress during the work day, whether it is using a company gym, eating healthier in the cafeteria or taking regular breaks. A study to be published in Population Health Management says “presenteeism,” which means people coming to work with physical or emotional problems, reduces productivity. The Salt Lake Tribune (Utah)
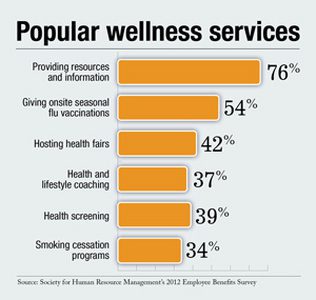
Some of the most popular wellness services offered are providing resources and information at 76 percent, giving onsite seasonal fluvaccinations at 54 percent and hosting health fairs at 42 percent. Other wellness efforts include health and lifestyle coaching at 37 percent, health screening at 39 percent and smoking cessation programs at 34 percent.
Considering that obesity and other chronic health issues continue to impact the well-being of employees and an employer’s bottom line, more respondents on a national level are offering lower health care premiums for getting an annual health risk assessment and not using tobacco according to surveys. The ROI on wellness is starting to pay – wellness plans pay for itself.
For more information, you may review the final rules in their entirety. For MMS Corp previous blogs on wellness, click here. we will keep you posted on future PPACA wellness program opportunities. In the meantime, please visit to view past blogs and Legislative Alerts at https://360peo.com/feed.
The views expressed in this post do not necessarily reflect the official policy, position, or opinions of MMS Corp. This update is provided for informational purposes. Please consult with a licensed accountant or attorney regarding any legal and tax matters discussed herein.