by admin | Nov 21, 2012
Average Base Policy Premiums by Age in 2012*
Age | 2012 Base Cost |
35 | $2,291.14 |
40 | $2,476.97 |
45 | $2,707.36 |
50 | $2,946.73 |
55 | $3,340.17 |
60 | $3,979.22 |
65 | $4,862.12 |
70 | $6,412.29 |
75 | $9,539.78 |
80 | $12,471.26 |
85 | $18,718.97 |
*Based on 3-6-50 Plan: 3 years nursing home or 6 years homecare or a combination of both where 2 homecare days is equal to 1 nursing home day.
Basic policies are those that are written to meet the minimum standards for the Partnership including:
- Minimum daily benefit amount of $253 for Nursing Home or $127 for home care including assisted living.
- Respite care 14 days per year
- Care Management 2 times per year
- Alternative level of care provided in a hospital
- Elimination period no great than 100 days
- 5% inflation protection
- Guaranteed renewal
- Extended Grace Period
- Denied Benefits Authorization Request are monitors by the Partnership
Please note: This is the average annual premium. Please shop wisely. Some companies’ premiums are lower and some are higher.
Some insurance companies offer reduced premiums for certain individuals, for example, discounts for spouses who each purchase a policy. Make sure you shop wisely before selecting your policy . Get Quote Here
All LTC premiums, generally speaking, remain constant starting with the premium at purchase and continuing year after year. In other words, your premium will not increase based on a decline in your health, advancing age, or other personal reasons . However, a future premium increase is possible if your insurance company requests this of t your State based on greater than expected claims experience.
by admin | Sep 27, 2012
Health Care Exchange
Example of Private Exchange here.
What is an Exchange? One of the centerpieces of the recently passed Patient Protection and Affordable Care Act
(PPACA) is the establishment of state based health insurance exchanges by the year 2014.
An “Exchange” is a mechanism for organizing the health insurance marketplace to help
consumers and small businesses shop for coverage in a way that permits easy comparison of
available plan options based on price, benefits, service and quality. By pooling individuals
and small groups together, transaction costs can be reduced and transparency can be increased.
Exchanges can create more efficient and competitive markets for individuals and small
employers.
Historically, the individual and small group health insurance markets have suffered from adverse
selection and high administrative costs, resulting in low value for consumers. “Exchanges” will
allow individuals and small businesses to benefit from the pooling of risk, market leverage, and
economies of scale that large businesses currently enjoy.
Beginning with an open enrollment period in 2013, Insurance agents and Benefits professionals
will help individuals and small employers shop, select, and enroll in high-quality, affordable
private health plans in these “Exchanges” to fit their specific needs at competitive prices.
Individuals in these “Exchanges” may also be eligible to receive premium subsidies through the
Federal or State government. By providing one-stop shopping, we will make purchasing health
insurance easier and more understandable through these “Exchanges” and provide the same level
of service that you have become accustomed to.
Middle-class people will be able to pick from a range of private insurance plans, and most people will be eligible for help from the government to pay their premiums.
Low-income people will be steered to safety-net programs for which they might qualify. This could be a problem in states that choose not to expand their Medicaid programs under a separate part of the health care law. In that case, many low-income residents in those states would remain uninsured.

Q: How will I know if I can get help with my health insurance premiums?
A: You’ll disclose your income to the exchange at the time you apply for coverage and they’ll let you know. Only legal residents of the United States can get financial assistance.
The health care law offers sliding-scale subsidies based on income for individuals and families making up to four times the federal poverty level, about $44,700 for singles, $92,200 for a family of four.
But do yourself a favor and read the fine print because the government’s help gets skimpier as household income increases.
For example, a family of four headed by a 40-year-old making $35,000 will get a $10,742 tax credit toward an annual premium of $12,130. They’d have to pay $1,388, about 4 percent of their income, or about $115 a month.
A similar hypothetical family making $90,000 will get a much smaller tax credit, $3,580, meaning they’d have to pay $8,550 of the same $12,130 policy. That works out to more than 9 percent of their income, or about $710 a month.
The estimates were made using the nonpartisan Kaiser Family Foundation’s online calculator. Some people will also be eligible for help with their copayments.
Final note: Though it’s called a “tax credit” the government assistance goes directly to the insurer. You won’t see a check.
Q: What will the benefits look like?
A: The coverage will be more comprehensive than what’s now typically available in the individual health insurance market, dominated by bare-bones plans. It will be more like what an established, successful small business offers its employees. Premiums are likely to be higher for some people, but government assistance should mostly compensate for that.
All plans in the exchange will have to cover a standard set of “essential health benefits,” including hospitalization, doctor visits, prescriptions, emergency room treatment, maternal and newborn care, and prevention. Insurers cannot turn away the sick or charge them more. Middle-aged and older adults can’t be charged more than three times what young people pay. Insurers can impose penalties on smokers.
Because the benefits will be similar, the biggest difference among plans will be something called “actuarial value.” A new term for consumers, it’s the share of expected health care costs that the plan will cover.
There will be four levels of coverage, from “bronze,” which will cover 60 percent of expected costs, to “platinum,” which will cover 90 percent. “Silver” and “gold” are in between. Bronze plans will charge the lowest premiums, but they’ll have the highest annual deductibles. Platinum plans will have the highest premiums and the lowest out-of-pocket cost sharing.
This part is insurance nerdy but an important point – The government’s subsidy will be tied to the premium for the second-lowest-cost plan at the silver coverage level that’s available in your area. You could take it and buy a lower cost bronze plan, saving money on premiums. But you’d have to be prepared for the higher annual deductible and copayments.
If you have additional questions regarding how SHOP Exchanges and Individual Exchanges can benefit you please contact our team at Millennium Medical Solutions Corp. Stay tuned for updates as more information gets released. We’re inside of 75 days until exchanges open, and information will be coming quickly in the next few months. Sign up for latest news updates.
Resource:
Click Above
Federal government health care site: www.healthcare.gov
Kaiser Health Reform Subsidy Calculator:http://healthreform.kff.org/subsidycalculator.aspx
Error: Contact form not found.

by admin | Sep 20, 2012 | family health insurance, Health Care Reform, NY News, Pharmaceutical Industry

Anti Mandatory Mail Order Victory. A little noticed NYS Healthcare Law has gone under the radar amidst fast changes in Affordable Care Act tumult. AMMO – Anti-Mandatory Mail Order passed late Dec 2011 effective for groups renewing after Jan 11, 2012. A significant signal by Governor Cuomo to stand up to the billion dollar industry no doubt.
According to trade group Pharmacists United for Truth the PBM (pharmaceutical benefits managemnt) claim that mandatory mail order lowers costs proves otherwisee. Plan sponsors are routinely charged far more than retail price in mandatory mail order plans, and their lack of transparency keeps plan sponsors to detecting the unreasonable prices.
After spending a good part of a day in early March helping a NYS client faced with mandatory mail order I learned of this change. For certain medications the insurer limits retail pharmacy coverage. While the incentivisation of 90 day supply at 2 copays was attractive this has now declined to 2.5 copay. With few exceptions such as specialty pharmaceuticals retail pharmacists are given the same advantages and evening the playing field.
The National Community Pharmacists Association’s blog post below offers a helpful FAQ. Additionally with the steady decline of the local independent pharmacist a quality of personalized care has been eroded. The price paid in patient compliance and safety has received little attention. Independent Pharmacists have been the canary in the mine for fellow small businesses competing with large copra big box chain stores. At least now NYS is finally listening.
By Kevin Schweers
Community pharmacists in New York scored a significant win for their patients, communities and pharmacy choice in late 2011 with the enactment of the Anti-Mandatory Mail Order or AMMO with overwhelming, bipartisan backing. What lessons might the campaign in support of the AMMO law hold for community pharmacists across the country?
To find out, NCPA recently asked one of the legislation’s staunchest supporters and advocates to share his observations on the effort to enact the AMMO law. Craig Burridge, M.S., is Executive Director of the Pharmacists Society of the State of New York (PSSNY). Mr. Burridge credits PSSNY members as most instrumental to enacting AMMO over the fierce opposition of mandatory mail order proponents, principally large pharmacy benefit managers (PBMs). He notes people including Ray Macioci, Charles Catalano, Vinny Chiffy and literally hundreds of pharmacy owners helped win a hard fought battle by gathering tens of thousands of signatures on petitions from their patients and coordinating tens of thousands of phone calls, emails and letters.
What follows is a Q&A with Mr. Burridge, in hopes that his advice would benefit patients and independent community pharmacists in other states advocating for patient choice.
NCPA: When it comes to the forced or mandated use of mail order pharmacies, many of the concerns expressed by patients and the community pharmacists who care for them are not new and have, in fact, been voiced for a number of years. What made 2011 different in New York?
Mr. Burridge: In New York, consumers by the tens of thousands signed petitions at their local pharmacy against mandatory mail order. Patients wrote dozens of letters to the editor of many regional newspapers telling about their horror stories with mail order. Finally, pharmacy owners had had enough of losing their patients to self-dealing PBMs. Tens of thousands of phone calls to the Governor’s Office and to Legislators were made by pharmacy owners, their staffs and their patients in support of passage of the no mandatory mail order bill.
NCPA: One obstacle to ensuring patient choice of pharmacy is the myth of mail order savings. This persists in some minds despite what appears to be rampant mail order waste and studies demonstrating how health plan sponsors that incent or require the use of mail order can end up paying more for drugs. Did you encounter such misperceptions and, if so, what did you do to alter or overcome them?
Mr. Burridge: We did in New York. The PBMs came at us with ads stating that costs would go up and that it was a ‘prescription drug tax’ or that it would ‘prohibit mail order.’ We responded with evidence that exposed the ‘spreads’ being used at mail for generics and the fact that the legislation requires participating pharmacies to agree to the same reimbursement and the same co-pays.
NCPA: The health care benefits of a patient’s face-to-face consultation with a community pharmacist and the preference of most patients for going to a local pharmacy are both well-established. But how did you chronicle and reinforce the economic and tax benefits of buying local when it comes to pharmacies?
Mr. Burridge: According to national data (IMS Health) for 2009, the last year we had data before introducing legislation, 22.8 percent of the national drug spend was for mail order prescriptions. Using New York’s percentage of total drug spend (11 percent), we removed hospital expenditures and Medicaid (which had less than one percent mail order) and came up with a mail order drug spend in NY in access of $5.8 billion annually. New York State has no major mail order facilities so this represents thousands of lost pharmacy jobs.
NCPA: Like PSSNY, NCPA continually stresses to its members the importance of grassroots activism, whether it is at the federal or state levels or with local employers and leaders. Did you find that your memberships became more engaged than usual in 2011 and, if so, what did you do to encourage their further involvement?
Mr. Burridge: It helped to have the PBM industry fly in colleagues from around the country and host their own Lobby Day. They told legislators that New York’s pharmacies could survive on acute medications only. This only caused yet another round of thousands of phone calls from our pharmacists, their staffs and patients. Our grass roots turned into a raging grass fire. Livelihoods were at stake and our opponents showed their hand. They wanted ALL maintenance medications going to their wholly-owned out-of-state mail order facilities. Our legislators saw that too.
NCPA: What surprised you the most about your 2011 campaign against mandatory mail order?
Mr. Burridge: I’ve been doing this too long to be surprised. We expected the worst from our opponents and they did not disappoint us.
NCPA: What were some of your opponents’ most challenging arguments and how did you address them?
Mr. Burridge: That depends if you consider outright lies as a challenge. Their ads said that it was a “Prescription Tax” or, when that flopped, they said our bill “would prohibit mail order.” These were easily swept aside and only upset legislators who felt the PBM industry was accusing them of passing a tax on prescription drugs.
NCPA: Do you have any other words of wisdom that you would like to share with concerned patients or your colleagues in community pharmacy?
Mr. Burridge: Choosing one’s pharmacy should be a basic right. If the playing field is level, it only makes sense to buy local. Watch out for PBMs calling all maintenance medications so-called ‘specialty drugs’ as a way of getting around no mandatory mail order laws. We’ll have a lot more to say on that in the near future.

by admin | Sep 20, 2012 | Health Care Reform
Lifetime and annual limits
In years past, most health insurance policies had limits or “caps” on the benefits they would pay. These limits were on any health plan participant (individual or family) – either over a lifetime or in a plan year. If someone exceeded that limit, benefits ended. While this rarely occurred, it resulted in major financial troubles for the few people it hit. The new law does not allow lifetime limits on”essential health benefits”. The law also restricts annual limits from now until 2014, when their use will become more limited. However, the law doesn’t prevent a plan from excluding all benefits for a condition.
Lifetime limits
Employers must eliminate lifetime limits on essential health benefits.
Effective
This applies to all health plans, including grandfathered plans.
Grandfathered plans will lose their grandfathered status if they impose an overall annual or lifetime limit on the dollar value of essential benefits if their plan did not include that limit prior to March 23, 2010. Plans can keep their grandfathered status if they convert lifetime limits into an annual limit at a dollar value that is lower than the lifetime limit on March 23, 2010.
Annual limits
Employers must eliminate annual limits by 2014. Until then, plans may place only “restrictive” annual limits on essential health benefits. The limits have been set for plan years that begin:
- 9/23/2010 to 9/22/2011 – $750,000 annual limit
- 9/23/2011 to 9/22/2012 – $1.25 million annual limit
- 9/23/2012 to 12/31/2013 – $2 million annual limit
Annual limits must apply on an individual-by-individual (not family) basis.
Essential Health Benefits defined
According to the law, the list of essential health benefits must include:
- Ambulatory patient services
- Emergency services
- Hospitalization
- Maternity and newborn care
- Mental health and substance use disorder services, including behavioral health treatment
- Prescription drugs
- Rehabilitative and habilitative services and devices
- Laboratory services
- Preventive and wellness services and chronic disease management
- Pediatric services, including oral and vision care
The government has not released the final regulation on essential benefits. Until it does, the government will take into account an employer’s “good faith effort” to comply with reasonable consistent interpretation.
by admin | Aug 30, 2012 | group health insurance, Health Care Reform, PPACA
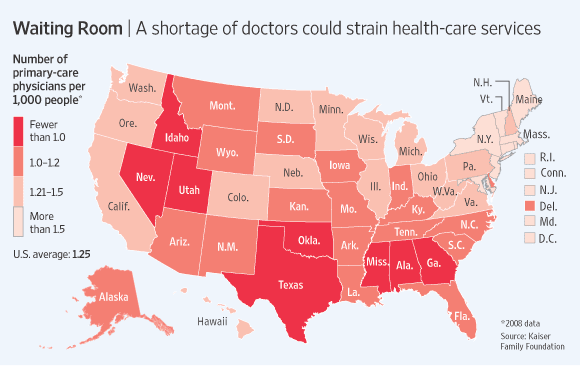
With increase in demand and already shortages of Doctors the Obamacare – Affordable Care Act will put significant severe strains on patient access.
According to todays WSJ article – John C. Goodman: Why the Doctor Can’t See You “Here is the problem: The health-care system can’t possibly deliver on the huge increase in demand for primary-care services. The original ObamaCare bill actually had a line item for increased doctor training. But this provision was zeroed out before passage, probably to keep down the cost of health reform. The result will be gridlock.”
The Department of Health and Human Services, estimated the minimum number of primary care physicians to ensure “adequate supply” at 60 to 80 per 100,000 population. By 2020 an estimated 45,000 new PCP would ne needed 2020. But the number of medical-school students entering family medicine fell more than a quarter between 2002 and 2007.
The greatest demand will be for primary-care physicians. These general practitioners, internists, family physicians and pediatricians will have a larger role under the new law, coordinating care for each patient.
“Take preventive care. ObamaCare says that health insurance must cover the tests and procedures recommended by the U.S. Preventive Services Task Force. What would that involve? In the American Journal of Public Health (2003), scholars at Duke University calculated that arranging for and counseling patients about all those screenings would require 1,773 hours of the average primary-care physician’s time each year, or 7.4 hours per working day.”
In 2014 an expected 30 Million people will be added The expected wait time would increase form 3 weeks to about 2 months. The 2 month estimate is a approximately how long it takes to schedule a check up in Boston which had enacted universal healthcare 5 years ago. Furthermore, the positive measures to encourage preventive care such as healthy screenings and well-care will only add to the gridlock.
“When people cannot find a primary-care physician who will see them in a reasonable length of time, all too often they go to hospital emergency rooms. Yet a 2007 study of California in the Annals of Emergency Medicine showed that up to 20% of the patients who entered an emergency room left without ever seeing a doctor, because they got tired of waiting.” Be prepared for that situation to get worse even with Urgent Care Centers.
“A New York Times survey of dermatologists in 2008 for example, found an extensive two-tiered system. For patients in need of services covered by Medicare, the typical wait to see a doctor was two or three weeks, and the appointments were made by answering machine.However, for Botox and other treatments not covered by Medicare (and for which patients pay the market price out of pocket), appointments to see those same doctors were often available on the same day, and they were made by live receptionists.”
As with any economic model the shorter supply of provider will drive up costs. Aside form provider fees increasing, those who can afford concierge service and pay $2,000-$4,000 may be able to get same day services and easy access but for most Americans with insurance will be waiting longer to see their Doctors. The irony is that people with coverage will have limited access to care.

by admin | Aug 14, 2012 | healthcare
Bluecard PPO – Outside members home region, the PPO medical plan is known as BlueCard PPO. The BlueCard plan offers a network of quality doctors and hospitals known as the BlueCard Provider Network.
- freedom to seek care in-network or out-of-network;
- no need to select a primary care physician to coordinate your care;
- visit specialists directly — no referrals are required;
- no claim forms to submit when using an in-network provider;
- no balance bills when using an in-nework provider;
- wellness programs, including fitness reimbursement and discounts on alternative health care services, at no additional cost;
- enhanced programs to control and manage chronic conditions;
- preventive care for children and adults;
- enjoy in-network coverage anywhere in the United States when you use providers that participate in the Personal Choice or BlueCard PPO networks;
- worldwide coverage and recognition of the Blue Cross® symbol.
How Does it Work?
Blank Suitcase Logo
A blank suitcase logo on a member’s ID card means that the patient has Blue Cross Blue Shield traditional, POS, or HMO benefits delivered through the BlueCard Program.
“PPO in a Suitcase” Logo
You’ll immediately recognize BlueCard PPO members by the special “PPO in a suitcase” logo on their membership card. BlueCard PPO members are Blue Cross and Blue Shield members whose PPO benefits are delivered through the BlueCard Program. It is important to remember that not all PPO members are BlueCard PPO members, only those whose membership cards carry this logo. BlueCard PPO members traveling or living outside of their Blue Plan’s area receive the PPO level of benefits when they obtain services from designated BlueCard PPO providers.

How to Verify Membership and Coverage
Once you’ve identified the alpha prefix, call BlueCard Eligibility to verify the patient’s eligibility and coverage.
 | 1. Have the member’s ID card ready when calling. |
| 2. Dial 1.800.676.BLUE. |
Operators are available to assist you weekdays during regular business hours (7am – 10pm EST). They will ask for the alpha prefix shown on the patient’s ID card and will connect you directly to the appropriate membership and coverage unit at the member’s Blue Cross Blue Shield Plan. If you call after hours, you will get a recorded message stating the business hours.
Keep in mind BCBS Plans are located throughout the country and may operate on a different time schedule than Anthem Blue Cross and Blue Shield. It is possible you will be transferred to a voice response system linked to customer enrollment and benefits or you may need to call back at a later time.
International Claims
The claim submission process for international Blue Cross and Blue Shield Plan members is the same as for domestic Blue Cross and Blue Shield Plan members. You should submit the claim directly to Anthem Blue Cross and Blue Shield.

by admin | Jun 25, 2012 | Health
Consider Supplements to Primary Medical Plans
Most are familiar with the AFLAC duck when it comes to supplemental benefits to primary medical plans. Today, primary medical plans are extremely valuable but in many cases the benefits paid cover only a fraction of the true cost of a major illness or injury. For instance, a person who suffers a severe heart attack can expect to experience a lengthy hospital stay, followed by a period of recuperation at home or in an extended care or rehabilitative facility. A primary medical plan will cover a significant portion of the hospital and physician costs, but the insured is likely to be responsible for some expenses. Depending on the terms of the plan, these expenses can be substantial. Most Popular Benefits The most in-demand voluntary benefits continue to be those that supplement core medical, life, or disability insurance coverage, according to surveys. These include dental, critical illness, specific illness, hospital supplemental, medical supplemental, disability buy-up, and supplemental life coverage. However, demographic trends are also contributing to growing interest in long-term care and financial planning products. As more people are faced with their parents’ elder care needs, they begin to appreciate the cost of extended care and anticipate what their needs may be in a few years. And, many mid-career employees face the double crunch of saving for retirement at the same time they are financing college education for their children. Perhaps reflecting the many demands on the time and money of today’s employees, 28 percent of participants in one survey said they wanted employers to provide a wider array of voluntary benefits. In addition, 30 percent of respondents said they were interested in having employer-provided access to financial planners to assist them in making decisions. |
Furthermore, an individual experiencing a health crisis such as a heart attack can expect to be absent from work for some time. A disability plan usually replaces only 60 percent to 70 percent of wages, and not everyone has disability coverage. This disruption to an individual’s income stream, combined with the added medical expenses, can devastate a family’s financial well-being, and can even force tough decisions about treatment options.
The prospect of experiencing a severe health calamity is not as uncommon as one might think. According to a study by the National Heart Lung and Blood Institute, 1.1 million Americans have heart attacks each year. And the American Cancer Society predicts more than 1.4 million new occurrences of cancer annually in the U.S., with men accounting for a slightly higher percentage than women.
Fortunately, insurance products are available that supplement a primary medical plan. Usually available to employees on a voluntary basis and at group rates, these products can fill gaps in traditional health insurance coverage such as the indirect costs of an illness or injury. Surprisingly, the indirect costs can sometimes outweigh the direct cost of medical care.
The following provides an overview of the types and benefits of supplemental medical insurance products. Remember that different carriers may market similar products under various names, and that the specific benefits provided may vary.
Critical illness insurance usually pays a cash benefit upon diagnosis of a life-threatening disease or condition, such as cancer, heart attack, stroke, or the need for an organ transplant. The benefit can be used as the insured — or survivors — see fit. For instance, the benefit may be used to pay for health care from an out-of-network provider under the primary plan; experimental treatment not covered by the primary plan; indirect costs associated with medical treatment, such as transportation, lodging, and child care; as well as lost income.
Some carriers offer disease-specific insurance. The most well known among these products is cancer insurance. Depending on the way the policy works, specific disease insurance may pay a cash benefit upon diagnosis, and/or may provide coverage beyond the primary medical plan for treatments associated with the disease, such as radiation and chemotherapy in the case of cancer insurance. Some cancer insurance carriers provide disease management services through a health care professional with expertise in oncology.
Catastrophe medical insurance provides coverage that kicks in after the primary medical plan has run out. Although many primary medical plans have high lifetime limits, some do not. This is especially true of those purchased with economy of premium in mind. Catastrophe plans carry a high deductible, but typically all medical expenses paid both by the insured and the insured’s primary plan count toward the deductible. In light of the high cost of health care, a low-limit primary plan can be easily exhausted. Consider the medical costs associated with a premature baby or the trauma of a major automobile accident. Catastrophe insurance provides much needed benefits for all of these types of occurrences.
Hospital indemnity insurance supplements the primary medical plan if an illness or injury requires a hospital stay. Depending on the policy terms, benefits may be paid for specified hospital procedures or on a cash per diem basis.
With today’s skyrocketing costs of medical care prompting employers to study how health insurance is offered to employees, voluntary supplemental medical coverage may be an appropriate offering for your workplace. Adding supplemental medical coverage to an umbrella of voluntary benefit offerings can bring value as well as flexibility to your employee benefit package. Remember that coverages vary by carrier, and by state. Speak with your insurance agent to learn which supplemental insurance products provide the coverages that best suit your needs.
For more information on how a work-site supplemental package would help you and your company please contact us at (855)667-4621 info@medicalsolutionscorp.com today.

by admin | May 30, 2012 | healthcare, Hospitals

Patients Waking Up To Major Colonoscopy Bill
The NYT article – Waking Up to Major Colonoscopy Bills illustartes what our clients are increasingly running into – increased out of pocket expenses.
“Patients who undergo colonoscopy usually receive anesthesia of some sort in order to “sleep” through the procedure. But as one Long Island couple discovered recently, it can be a very expensive nap. Both husband and wife selected gastroenterologists who participated in their insurance plan to perform their cancer screenings. … And in both cases, the Gastroenterologists were assisted in the procedure by anesthesiologists who were not covered by the couple’s insurance. They billed the couple’s insurance at rates far higher than any plan would reimburse — two to four times as high, experts say.”
Patients can go for Colonoscopies either in an outpatient medical office or in ambulatory hospital setting. Gastrointerologists cannot bill for the anesthesia unless there is an employed licensed Anesthesiologist on staff. The treating Physician cannot be the same person who administer/monitors the sedation. Generally speaking the Anesthesiologist in a hospital settings are separate entities and attempt to bill independently form the hospital charges. Now you can begin to see how patients are getting added billing.
Furthermore, we are seeing increasing out of network charges with Physicians dropping health plans in certain geographic areas as well as insurers shifting more of the costs burden.
The posting Out of Control Out of Network Charges points to examples such as – “a neurosurgeon charged $159,000 for an emergency procedure for which Medicare would have paid only $8,493.” Another example: “ a consumer went to an in-network hospital for gallbladder surgery with a participating surgeon. The consumer was not informed that a non-participating anesthesiologist would be used, and was stuck with a $1,800 bill. Providers are not currently required to disclose before they provide services whether they are in-network.” The average out-of-network radiology bill was 33 times what Medicare pays, officials say.
Our clients get 3 bills with any procedure needing general anesthesia
1) A bill from the hospital
2) A bill from the surgeon
3) A bill from anesthesia
Actually, the physician bill is typically the lowest cost of the bill . On a $5,000 total bill the GI may only get 10%. Sometimes the hospital and anesthesia charges are bundled into a single bill but many times they are not. On most plans patients can negotiate with the hospital depending on pre-authorization the anesthesia bill and resubmit charges. This is probably the most common appeal we perform on behalf of our clients.
Patient on a cost sharing plan with in-network deductibles may fair better with outpatient office colonoscopies. From an insurer costs perspective the charges in an office setting are typically $2,000-$2,500. So why do it in the hospital? The procedure may require general anesthesia and financial incentives. Also, at times the procedure may be a loss to the provider. For example, Pediatricians will not perform Gardasil vaccination because the vaccine costs more than what the pediatrician will get reimbursed to give it.
The vast majority of providers make sure that patients were in-network or arranged pre-payment plan prior to the procedure. As with most non-HMO plans, however, the responsibility rests with patient to make sure everything is pre-authorized and in network is possible.

 Doctor Shortages-covered but less access?
Doctor Shortages-covered but less access?