Recently, UHC/Oxford and Mt Sinai Health System had split effective January 1, 2024. Since that time there have been a state-required cooling-off period and ongoing talks on resolution but that has not yielded a positive outcome yet. The Mount Sinai Hospital, Mount Sinai Queens, and their related hospital outpatient locations will remain in-network for all patients until at least Friday, March 1.
According to UnitedHealthcare/Oxford:
People enrolled in UnitedHealthcare fully insured commercial plans have continued network access to all of Mount Sinai’s hospitals through Feb. 29, 2024, due to New York cooling-off requirements.
Unless they obtain admitting privileges to another in-network hospital, the majority of Mount Sinai’s physicians will no longer participate in our network for employer-sponsored and individual plans, including the Oxford Health Plan, effective March 22, 2024.
This negotiation only impacts our relationship with Mount Sinai for employer-sponsored and individual commercial plans, including Oxford. All other active contracts, including Medicare Advantage and the Empire Plan, remain in place with no change.
The two organizations had a three-year agreement that took effect on Jan. 1, 2022, which was canceled before it was supposed to expire amid a dispute over payment rates. Both institutions are blaming one another for the standoff.
Mount Sinai claims UnitedHealthcare compensates it an average of 30% less for care than other health systems in New York. The insurer pays New York-Presbyterian $25,911 for a normal vaginal birth, and Mount Sinai $15,989, Mount Sinai said.
“Mount Sinai must be paid fairly,” spokeswoman Lucia Lee said in a statement. “As Mount Sinai costs substantially less than our peers, UHC/Oxford will actually end up paying more for patients to get care at other systems in New York. This cost — estimated to be at least $140 million more over the course of a year — will be passed on to employers and patients.”
UnitedHealthcare says Mount Sinai sought “outlandish price hikes” that would increase costs for services an average of 50% over three years or $600 million — an estimate disputed by Mount Sinai. For example, a regular, outpatient colonoscopy at South Nassau costs about $6,000 and would be about $8,700 in three years under Mount Sinai’s proposal, according to UnitedHealthcare.
Mt Sinai Hospitals & Health System
Facility Name
County
Mount Sinai Beth Israel
NYC
The Mount Sinai Hospital
NYC
Mount Sinai Morningside
NYC
The Mount Sinai West
NYC
Mount Sinai-Union Square
NYC
Mount Sinai Kravis Children’s Hospital
NYC
Mount Sinai-Behavioral Health Center (MSBHC)
NYC
Blavatnik Center, Medical Center
NYC
New York Eye and Ear Infirmary of Mount Sinai
NYC
Mount Sinai Brooklyn
Brooklyn
Mount Sinai Queens
Queens
Mount Sinai South Nassau
Long Island
Neighboring Hospitals
Bellevue Hospital Center
NYC
New York Presbyterian Queens
Queens
Elmhurst Hospital Center
Queens
New York Presbyterian Weill Cornell
NYC
Flushing Hospital Medical Center
Queens
North Shore University Hospital Manhasset
Long Island
Lenox Hill Hospital
NYC
NYU Langone Hospital Brooklyn
Brooklyn
Long Island Jewish Medical Center
Brooklyn
NYU Langone Hospital Long Island
Long Island
Maimonides Medical Center
Brooklyn
St. Francis Hospital
Long Island
Mercy Medical Center
Long Island
St. Johns Episcopal Hospital
Queens
New York Presbyterian Columbia
NYC
St. Joseph Hospital
Queens
New York Presbyterian Lower Manhattan Hospital
NYC
Wyckoff Heights Medical Center
Brooklyn
Both sides need each other as both are market leaders in their fields. It is our hope and most of our clients that they get this resolved soon. In the meantime, please bookmark our site for the latest updates. And do reach out to us and learn the steps that you can take to smoothen this temporary roadblock.
We already love Professional Employer Organizations (PEO)– our clients do too. Today we’re counting down our top 5 reasons why we love PEO:
1. National Capabilities: It ensures your compliance with local and federal laws, even if your business has locations in different states. Access to a national provider healthcare plan, not single state carriers
2. Liability Protections: Some liability moves to the PEO service instead of your company.
3. It saves you money on HR staff. Being part of a PEO gives you a clear-cut idea of what your costs are going to be a year in and year out. The PEOs work tirelessly to keep their insurance renewals down, so their clients won’t leave. Every year they work with the insurance carriers to introduce new plans and ways to reduce the costs of insurance to their clients. This gives you the ability to forecast and know precisely what your costs will be.
4. Technologies: Online HR resources for self-service issues Ability for employees to make personal changes on their own, online. Ability to track PTO (paid-time off).
5. One Vendor: It streamlines HR tasks like payroll, taxes, employee benefits, worker’s compensation, 401K, and HR administrative tasks.
Our PEO Quoting Tool ensures that we have first-hand insight as to what the small business owner needs to be successful. Click below for a quote.
Healthcare is constantly evolving, shaping how people view their health and well-being. The complexities of managing rising healthcare costs, the continuous evolution of the modern workplace, and a heightened focus on employee wellbeing highlight the necessity for a broader perspective on the concept of “workplace wellbeing.”
To be successful, organizations must construct a future that works for everyone, including individuals, the workforce, and the organization.
How will employers invest in workplace well-being?
According to aGreat Place to Workand Johns Hopkins survey in 2023, employee well-being is a key predictor of employee retention and referrals. It identifies that:
Promoting employee well-being requires consistent listening and regular communication with employees.
Employees who experience high levels of well-being in the workplace are three times more likely to stay with their employer.
Employees who experience high levels of well-being in the workplace are three times more likely to recommend their employer to others.
It’s safe to say that providing a culture of health and well-being within your organization significantly impacts more than just healthcare costs and physical health.
Think about every aspect of your life where support is needed—and how everyone’s list differs. Wellbeing at work should be addressed by supporting the “whole person.” This means employers should support not only physical health but also the following:
Mental health
Digital wellbeing
A work-life balance
Financial wellbeing
Family support services
Although this list is not exhaustive, it highlights the complex and interdependent nature of workplace wellbeing needs.
5 trends that will shape the future of employee wellbeing:
Mental Health and Emotional Wellbeing:
Emotional wellbeing has taken center stage in the post-pandemic years. One positive outcome of the pandemic is the awareness and need for greater mental health resources and the de-stigmatization of mental health in the workplace. According to aGallup poll, 19% of U.S. workers rate their mental health as fair or poor.
Here are some of the things that are being implemented as they relate to mental wellbeing at work:
“Safe Space” communities:Employees can access mental health resources and learn to support others while sharing personal stories.
Manager’s Training:Leaders can access training to learn how to be effective listeners, identify, and respond swiftly to the mental health needs of their teams. These training courses also help inform company policy needs and provide a framework to be developed within all areas of the organization.
Mindfulness Resources:Incorporating relaxation solutions into the workplace with on-the-go apps, online platforms, calm spaces, or meditation rooms involves integrating mindfulness tools into communication platforms.
The Continued Rise of Technology – Driven Solutions
The intersection of convenience, privacy, and adaptability is crucial for digital wellbeing tools. Integrating technology into employee wellbeing programs not only improves accessibility and convenience but also enhances data collection and analysis, which helps organizations gain insight into health trends and potential interventions. Finding a way to tie these different technology systems together will be instrumental when it comes to the interconnectedness of data and programs.
Some solutions are determined to stick around, and ones that you might consider include:
Personalized Wellness Platforms: Artificial Intelligence (AI) is inspired to adapt to individual preferences and circumstances with constantly evolving algorithms that adjust real-time recommendations based on new user data, behavioral patterns, personalized content, and customized plans.
Telehealth Solutions: With multi-modal consultation formats and interactive platforms, integrated health allows individual solutions to be consolidated into more holistic platforms, bringing together everything someone needs in one place.
Wearable Technology: Fitness trackers and smartwatches are being used to monitor physical activity, sleep patterns, and overall health. Wearables that adapt their tracking based on user lifestyle algorithms will be instrumental in personalization and customization.
Flexibility and Work/Life Balance:
The COVID-19 pandemic forced organizations to adopt remote work arrangements on an unprecedented scale. Whether your office now promotes a worksite that is hybrid, in-office, or remote, having flexible work arrangements helps accommodate employees, enhance work-life balance, and make companies more attractive.
Develop strategies to support employees wherever they are:
Virtual Wellness and Fitness Classes:Allow employees to participate in their health and wellbeing wherever they are.
Telehealth Visits:Offers flexibility to talk with a doctor from the comfort of their home.
Virtual Team-building Activities:Allow employees to connect even though they are not physically together.
Invest in Technology Tools:Facilitating seamless collaboration among remote and in-office teams or multiple locations.
Financial Wellbeing
A recentstudy by PwCfound that57%of employees say finances are the top cause of stress in their lives. When people have money worries, it impacts morale and productivity, not to mention overall physical and mental health. Businesses have a responsibility to help their employees by investing in financial wellbeing, education, and resources, but also to help retain top talent in this ever-changing job market.
Here are some services to consider offering:
Financial Wellness Coaching:Such as one-on-one coaching, workshops, webinars, and online tools
Financial Education:Literacy opportunities on topics such as budgeting, saving, investing, debt management, and overall financial planning.
Financial Wellness Benefits:Such as tuition reimbursement, employer-sponsored retirement plans, or home-buying assistance programs.
Family Support Services:
Balancing the roles of parent, caregiver, and employee can feel like juggling two full-time jobs. Having a supportive employer makes all the difference.Caregiver responsibilitiesfor both children and aging parents put a strain on mental and physical health. Having programs and support for a range of needs helps employees feel supported.
How do you invest in caregivers?
Financial support, such as childcare subsidies or discounts for daycare centers
Flex spending accounts for dependent care expenses
Backup care services
Eldercare resources
Caregiver leave/paid time off
Maternity and paternity leave
Mental health benefits for caregivers
Return to work programs
Wellbeing investments in the workplace are retention boosters and help secure top talent. According to anotherGallup poll, 63% of workers say that having work-life balance and better personal wellbeing opportunities is very important when considering a new job. Organizations should look to provide more inclusive, equitable benefits and wellbeing programs across their workforce. In the future, organizations will intensify their focus on human-centric wellbeing, aiming to enhance the employee experience and drive concrete business results by evolving from the appearance of personalization to genuine personalization.
The wellness landscape is changing daily. Employers should research the options by seeking guidance with a PEO. We have multiple wellness programs and initiatives that can be implemented and offer comprehensive ACA compliance/reporting services to clients.
This Compliance Overview is not intended to be exhaustive nor should any discussion or opinions be construed as legal advice. Readers should contact legal counsel for legal advice.
In preparation for open enrollment, Employers should review their plan documents in light of changes for the plan year beginning Jan 1, 2024. Below is an Employer 2024 Open Enrollment Checklist including some administrative items to prepare for in 2024.
Change has been constant for employer plans in the last few years. Unfortunately, 2023 was no exception. As they prepare for 2024 open enrollment, employers must incorporate new requirements affecting the design and administration of their health plans for plan years beginning on or after Jan. 1, 2024. Those changes include items that are adjusted for cost of living changes each year, – e.g., the cost-sharing limits for high deductible health plans (HDHPs), contribution limits to health savings accounts (HSAs), as well as new requirements due to legislative and regulatory updates, such as the expiration of COVID-19 mandates, to name a few.
Employers should ensure their health plan is updated and communicate benefit changes to participants through an updated summary plan description (SPD) or a summary of material modifications (SMM) for the 2024 plan year.
As a general best practice, employers should confirm that their open enrollment materials contain certain required participant notices and consider including some periodic notices, such as the Medicare Part D creditable/non-creditable coverage notice, in their open enrollment materials.
PLAN DESIGN CHANGES
ACA Mandates
Affordability Requirements
Under the ACA’s employer shared responsibility rules (the “pay or play” rules), applicable large employers (ALEs) (those with 50 or more full-time employees or the equivalent) are required to offer affordable, minimum value health coverage to their full-time employees (and dependent children) or risk paying a penalty.
Under the ACA, an ALE’s health coverage is considered affordable if the employee’s required contribution to the plan does not exceed 9.5% of the employee’s household income for the taxable year (as adjusted each year). The adjusted percentage is 9.12% for 2023.
The affordability percentage for plan years that begin on or after Jan. 1, 2024, will be 8.39%. That is another reduction demonstrating the need for ALEs to monitor the affordability percentage each year so they can confirm that at least one of the health plans offered to full-time employees satisfies the ACA’s affordability standard (typically by the use of one of the optional safe harbors – federal poverty level, W-2 or rate of pay).
Out-of-pocket Maximum
Under the ACA, non-grandfathered health plans (which apply to almost all employer plans) are subject to limits on cost sharing for essential health benefits. Confirm that out-of-pocket maximum limits for your health plan comply with the ACA’s limits for the 2024 plan year.
Plan years beginning on or after Jan. 1, 2024:
$9,450for self-only coverage
$18,900for family coverage
Note, the out-of-pocket maximum limits for HDHPs compatible with HSAs must be lower than the ACA’s limits. For the 2024 plan year, the out-of-pocket maximum limits for HDHPs are $8,050 for self-only coverage and $16,100 for family coverage.
Preventive Care Benefits
The ACA requires non-grandfathered health plans to cover certain preventive health services without imposing cost-sharing requirements (e.g., deductibles, copayments, or coinsurance) when in-network healthcare providers supply the services. The preventive care services covered by the requirements are based on the following:
Evidence-based items or services that have a rating of A or B in the current recommendations of the United States Preventive Services Task Force (USPSTF).
Immunizations for routine use in children, adolescents, and adults that are currently recommended by the Centers for Disease Control and Prevention.
Evidence-informed preventive care and screenings are included in the Health Resources and Services Administration (HRSA) guidelines for infants, children, and adolescents.
Evidence-informed preventive care and screenings are included in HRSA-supported guidelines for women.
There needs to be some clarity. An ongoing court case has raised some uncertainty about using the USPSTF recommendations. However, guidance from federal agencies will permit employers to use those factors without the risk of penalties for the time being. Therefore, employers should monitor future developments regarding the ACA’s preventive care mandate, which is expected by the end of 2023.
Coverage For COVID-19 Vaccines, Testing And Treatment
Because the COVID-19 public health emergency has ended (seeAlert here), health plans are no longer required to cover COVID-19 diagnostic tests and related services without cost sharing or other medical management requirements. Health plans are still required to cover recommended preventive services (under the ACA requirements), including COVID-19 immunizations, without cost sharing, but this coverage requirement can now be limited to in-network providers.
For plan years ending after Dec. 31, 2024, an HSA-compatible HDHP is no longer permitted to provide COVID-19 testing and treatment benefits without a deductible (or with a deductible below the minimum deductible for an HDHP). Therefore, employers should
Determine whether health plans will impose cost-sharing requirements, prior authorization, or other medical management requirements on COVID-19 testing for the upcoming plan year.
Determine whether health plans will continue covering COVID-19 immunizations without cost sharing from all healthcare providers or whether this first-dollar coverage will be limited to in-network providers.
Confirm that HDHPs that do not have a calendar year as the plan year will not pay benefits for COVID-19 testing and treatment before the annual minimum deductible has been met for plan years ending after Dec. 31, 2024.
Notify plan participants of any changes for the 2024 plan year regarding COVID-19 testing and vaccines through an updated SPD or SMM.
The IRS issued a memorandum on claims substantiation (see Article here) for health FSAs. The memorandum clarifies that health FSA expenses are not considered properly substantiated if employees self-certify expenses, if the plan uses sampling, if only amounts over a certain level are substantiated, or if charges from favored providers are not substantiated. Employers should, therefore, review the health FSA substantiation procedures to make sure they comply with IRS rules.
If you offer an HDHP to your employees that is compatible with an HSA, you should confirm that the HDHP’s minimum deductible and out-of-pocket maximum comply with the 2020 limits. The IRS limits for HSA contributions and HDHP cost-sharing increase for 2024. The HSA contribution limits will increase effective Jan. 1, 2024, while the HDHP limits will increase effective for plan years beginning on or after Jan. 1, 2024.
Check whether your HDHP’s cost-sharing limits need to be adjusted for the 2024 limits.
If you communicate the HSA contribution limits to employees as part of the enrollment process, these enrollment materials should be updated to reflect the increased limits that apply for 2024.
The following table contains the HDHP and HSA limits for 2024 as compared to 2023. It also includes the catch-up contribution limit that applies to HSA-eligible individuals who are age 55 or older, which is not adjusted for inflation and stays the same from year to year.
Type of Limit
2024
2023
Change
HSA Contribution Limit
Self-only
$4,150
$3,850
Up $300
Family
$8,300
$7,750
Up $550
HSA Catch-up Contributions (not subject to adjustment for inflation)
Age 55 or older
$1,000
$1,000
No change
HDHP Minimum Deductible
Self-only
$1,600
$1,500
Up $100
Family
$3,200
$3,000
Up $200
HDHP Maximum Out-of-pocket Expense Limit (deductibles, copayments and other amounts, but not premiums)
Self-only
$8,050
$7,500
Up $550
Family
$16,100
$15,000
Up $1,100
HDHP Design Option – Telehealth
At the beginning of the COVID-19 pandemic, Congress temporarily relaxed the rules for HDHPs to allow them to provide benefits for telehealth or other remote care services before plan deductibles were met without jeopardizing HSA eligibility. That relaxed rule currently applies for plan years beginning before Jan. 1, 2025.
Determine whether HDHPs will waive the deductible for telehealth services for the plan year beginning in 2024
Communicate plan changes for the upcoming year to participants through an updated SPD or SMM
Mental Health Parity – Required Comparative Analysis For NQTLs
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires parity between a group health plan’s medical/surgical benefits and its mental health or substance use disorder (MH/SUD) benefits. These parity requirements apply to financial requirements and treatment limits for MH/SUD benefits. In addition, any nonquantitative treatment limitations (NQTLs) placed on MH/SUD benefits must comply with MHPAEA’s parity requirements. For example, NQTLs include prior authorization, step therapy protocols, network adequacy, and medical necessity criteria.
MHPAEA requires health plans and issuers to conduct comparative analyses of the NQTLs used for medical/surgical benefits compared to MH/SUD benefits. This analysis must contain a detailed, written, and reasoned explanation of the specific plan terms and practices and include the basis for the plan or issuer’s conclusion that the NQTLs comply with MHPAEA. Plans and issuers must make their comparative analyses available to specific federal agencies or applicable state authorities upon request.
Employers should request that health plan issuers (or third-party administrators) confirm that comparative analyses of NQTLs will be updated, if necessary, for the plan year beginning in 2024 and make the analysis available to the employee.
Open Enrollment Notices
Employers who sponsor group health plans should provide certain benefits notices in connection with their open enrollment periods. Some of these notices must be provided at open enrollment time, such as the Summary of Benefit and Coverage (SBC). Other notices, such as the WHCRA notice, must be distributed annually. Although these annual notices may be provided at different times throughout the year, employers often include them in their open enrollment materials for administrative convenience.
In addition, employers should review their open enrollment materials to confirm that they accurately reflect the terms and cost of coverage. In general, any plan design changes for 2024 should be communicated to plan participants through an updated SPD or an SMM.
Summary Of Benefits And Coverage
The ACA requires health plans and health insurance issuers to provide an SBC to applicants and enrollees each year at open enrollment or renewal. Federal agencies have provided atemplatefor the SBC, which health plans must use.
Note that for self-funded plans, the plan administrator is responsible for providing the SBC. For insured plans, the issuer usually prepares the SBC. If the issuer prepares the SBC, an employer is not required to also prepare an SBC for the health plan, although the employer may need to distribute the SBC prepared by the issuer.
Medicare Part D Notices
Group health plan sponsors must provide a notice of creditable or non-creditable prescription drug coverage to Medicare Part D-eligible individuals covered by, or who apply for, prescription drug coverage under the health plan. The notice alerts the individuals about whether their prescription drug coverage is at least as good as Medicare Part D coverage. The notice generally must be provided at various times that cannot always be anticipated, including when an individual enrolls in the plan and each year before Oct. 15 (when the Medicare annual open enrollment period begins). Therefore, the best practice is to provide it annually at open enrollment, as that will ensure timely compliance. Model notices are available on the Centers for Medicare and Medicaid Services’website.
Annual CHIP Notices
Group health plans covering residents in a state that provides a premium subsidy to low-income children and their families to help pay for employer-sponsored coverage must send an annual Children’s Health Insurance Program (CHIP) notice about the available assistance to all employees in that state. The U.S. Department of Labor (DOL) has provideda model notice.
Initial COBRA Notices
COBRA applies to employers with 20 or more employees who sponsor group health plans. Group health plan administrators must provide an initial COBRA notice to new participants and certain dependents within 90 days after plan coverage begins. The initial COBRA notice may be incorporated into the plan’s SPD. Because the COBRA election-period will not start until this notice is provided, it is helpful to many employers to include a copy in the open enrollment materials as a backup.
Notices Of Patient Protections
Under the ACA, group health plans and issuers that require the designation of a participating primary care provider must permit each participant, beneficiary, and enrollee to designate any available participating primary care provider (including a pediatrician for children). Additionally, plans and issuers that provide obstetrical/gynecological care and require a designation of a participating primary care provider may not require preauthorization or referral for such care. If a health plan requires participants to designate a participating primary care provider, the plan or issuer must provide a notice of these patient protections whenever the SPD or similar description of benefits is provided to a participant. If an employer’s plan is subject to this notice requirement, they should confirm that it is included in the plan’s open enrollment materials. This notice may be included in the plan’s SPD.Model languageis available from the DOL.
Grandfathered Plan Notices
If an employer has a grandfathered plan, they should include information about its grandfathered status in plan materials describing the coverage under the plan, such as SPDs and open enrollment materials. Model language is available from the DOL.
Notices Of HIPAA Special Enrollment Rights
At or before enrollment, an employer’s group health plan must provide each eligible employee with a notice of their special enrollment rights under HIPAA. This notice may be included in the plan’s SPD.
HIPAA Privacy Notices
The HIPAA Privacy Rule requires covered entities (including group health plans and issuers) to provide a Notice of Privacy Practices (or Privacy Notice) to everyone who is the subject of protected health information (PHI). Health plans are required to send the Privacy Notice at certain times, including to new enrollees at the time of enrollment. Also, at least once every three years, health plans must either redistribute the Privacy Notice or notify participants that the Privacy Notice is available and explain how to obtain a copy. Self-insured health plans are required to maintain and provide their own Privacy Notices. However, special rules apply for fully insured plans, where the health insurance issuer, not the plan itself, is primarily responsible for the Privacy Notice.
Special Rules for Fully Insured Plans
The plan sponsor of a fully insured health plan has limited responsibilities with respect to the Privacy Notice, including the following:
If the sponsor of a fully insured plan has access to PHI for plan administrative functions, they are required to maintain a Privacy Notice and to provide the notice upon request.
If the sponsor of a fully insured plan does not have access to PHI for plan administrative functions, they are not required to maintain or provide a Privacy Notice.
A plan sponsor’s access to enrollment information, summary health information, and PHI that is released pursuant to a HIPAA authorization does not qualify as having access to PHI for plan administration purposes.
Model Privacy Notices are available through the Department of Health and Human Services.
WHCRA Notices
Plans and issuers must provide notice of participants’ rights to mastectomy-related benefits under the WHCRA at the time of enrollment and annually. The DOL’s compliance assistance guide includes model language for this disclosure.
SARs
Plan administrators required to file Form 5500 must provide participants with a narrative summary of the information in Form 5500, called a summary annual report (SAR). Amodel noticeis available from the DOL.
Group health plans that are unfunded (that is, benefits are payable from the employer’s general assets and not through an insurance policy or trust) are not subject to the SAR requirement. The plan administrator generally must provide the SAR within nine months of the close of the plan year. If an extension of time to file Form 5500 is obtained, the plan administrator must furnish the SAR within two months after the close of the extension period.
Wellness Program Notices
Group health plans that include wellness programs may be required to provide certain notices regarding the program’s design. As a general rule, these notices should be provided when the wellness program is communicated to employees and before employees provide any health-related information or undergo medical examinations. These notices are required in the following situations:
HIPAA Wellness Program Notice—HIPAA imposes a notice requirement on health-contingent wellness programs offered under group health plans. Health-contingent wellness plans require individuals to satisfy standards related to health factors (e.g., not smoking) to obtain rewards. The notice must disclose the availability of a reasonable alternative standard to qualify for the reward (and, if applicable, the possibility of waiver of the otherwise applicable standard) in all plan materials describing the terms of a health-contingent wellness program. The DOL’scompliance assistance guideincludes a model notice that can be used to satisfy this requirement.
ADA Wellness Program Notice—Employers with 15 or more employees are subject to the Americans with Disabilities Act (ADA). Wellness programs that include health-related questions or medical exams must comply with the ADA’s requirements, including an employee notice requirement. Employers must give participating employees a notice that tells them what information will be collected as part of the wellness program, with whom it will be shared, and for what purpose, as well as the limits on disclosure and the way information will be kept confidential. The U.S. Equal Employment Opportunity Commission (EEOC) has provided asample noticeto help employers comply with this ADA requirement.
ICHRA Notices
Employers may use individual coverage HRAs (ICHRAs) to reimburse their eligible employees for insurance policies purchased in the individual market or Medicare premiums. Employers with ICHRAs must notify eligible participants about the ICHRA and its interaction with the ACA’s premium tax credit. In general, this notice must be provided at least 90 days before the start of each plan year. Employers may provide this notice at open enrollment time if it is at least 90 days before the beginning of the plan year. A model notice is available for employers to use to satisfy this notice requirement.
________________________________
Enhance Your Employee Benefits Package. A competitive benefits package is key to keeping and attracting top talent.Assess your current benefits package and consider making necessary adjustments to include options, such as expanded mental health support, for example.
GENERAL HR
Review Employee Records. The fourth quarter is a good time to review your employee records and check record retention guidelines. Don’t forget to dispose of outdated termination and outdated job applications properly. With W2s around the corner, make sure all addresses and information are updated.
Develop and Distribute Your 2024 Calendar. Create and distribute a calendar outlining important dates, vacation time, pay dates, and company-observed holidays for 2024.
Review and Update Employee Handbook. Review your employee handbook to make sure it is up-to-date and addresses areas, such as employment law mandates, new COVID-related policies, guidelines for remote working, privacy policies, compensation and performance reviews, social media policies, attendance, and time-off, break periods, benefits, and procedures for termination, discipline, workplace safety, and emergency procedures.
PLEASE NOTE: This Checklist is not intended to be exhaustive nor should any discussion or opinions be construed as legal advice. Readers should contact legal counsel for legal advice. This information is for general reference purposes only. Because laws, regulations, and filing deadlines are likely to change, please check with the appropriate organizations or government agencies for the latest information and consult your employment attorney and/or benefits advisor regarding your responsibilities. In addition, your business may be exempt from certain requirements and/or be subject to different requirements under the laws of your state. (Updated Sept 3, 2023)
Contact us at (855) 667-4621 or email us at info@360peo.com
About this Session: Engaging your workforce and captivating them: How do you achieve this? During this session we discuss how to deploy engaging tactics with the right balance of frequency and educational impacts across a multi-generational workforce to engage your employees when it matters most..
Why We Love PEO This Valentine’s Day. Today we’re counting down our top 5 reasons why we love PEO. National Capabilities, Liability Protections, Technologies, One Vendor and PEO saves you money on HR staff. Try Our PEO Quoting Tool today.
Discover the future of employee wellbeing. From mental health strategies to tech-driven solutions and flexible work arrangements, this piece explores 5 trends shaping the workplace of tomorrow.
“This year’s rankings represent an expanded universe, with three new countries on the list—Colombia, Saudi Arabia, and the United Arab Emirates—bringing the total to over 2,300 hospitals in 28 countries. And the results show a remarkable cross-section of excellence across the world: Twenty-one countries are represented in the global top 150. The U.S. leads with 29 hospitals, followed by Germany with 16; Italy and France with 10 each; and South Korea with eight. Overall, there were 13 new hospitals in this year’s top 100. Among the biggest movers from last year’s rankings were No. 8 Northwestern Memorial Hospital (28 in 2022); No. 40 Seoul’s Samsung Medical Center (73) and No. 11 New York’s NYU Langone Hospitals (59).”
Top 10 Internationally:
1Mayo Clinic Rochester- United States 2Cleveland Clinic- United States 3Massachusetts General Hospital- United States 4The Johns Hopkins Hospital- United States 5Toronto General – University Health Network- Canada 6Karolinska Universitetssjukhuset- Sweden 7Charité – Universitätsmedizin- BerlinGermany 8AP-HP – Hôpital Universitaire Pitié Salpêtrière- France 9Singapore General Hospital- Singapore 10UCLA Health – Ronald Reagan Medical Center- United States
Top 20 Nationally:
1Mayo Clinic – Rochester 2ClevelandClinic 3MassachusettsGeneral Hospital 4TheJohns Hopkins Hospital 5UCLAHealth – Ronald Reagan Medical Center 6 Stanford Health Care – Stanford Hospital 7BrighamAnd Women’s Hospital 8NorthwesternMemorial Hospital 9TheMount Sinai Hospital 10New York-Presbyterian Hospital-Columbia and Cornell
11. University of Michigan Hospitals – Michigan Medicine 12 Cedars-Sinai Medical Center 13. UCSF Medical Center 14. Duke University Hospital 15. Hospital of the University of Pennsylvania – Penn Presbyterian 16. NYU Langone Hospitals 17. Mayo Clinic – Jacksonville 18. Russh University Medical Center 19. Mayo Clinic – Phoenix 20. Houston Methodist Hospital
Top 10 NY/NJ Metro Hospitals:
9
The Mount Sinai Hospital
83.98%
New York
NY
10
New York-Presbyterian Hospital-Columbia and Cornell
83.94%
New York
NY
16
NYU Langone Hospitals
81.23%
New York
NY
46
Morristown Medical Center
70.66%
Morristown
NJ
57
Hackensack University Medical Center
69.52%
Hackensack
NJ
117
Strong Memorial Hospital – University of Rochester
65.36%
Rochester
NY
121
Valley Hospital
65.30%
Ridgewood
NJ
130
North Shore University Hospital
65.21%
Manhasset
NY
148
Saratoga Hospital
64.71%
Saratoga Springs
NY
167
Overlook Medical Center
64.42%
Summit
NJ
Top 3 CT Hospitals:
35YaleNew Haven Hospital 158 St. Francis Hospital& Medical Center 201Griffin Hospital
Top 10 PA Hospitals:
15
Hospital of the University of Pennsylvania – Penn Presbyterian
Philadelphia
PA
54
Jefferson Health – Thomas Jefferson University Hospitals
Philadelphia
PA
58
UPMC Presbyterian & Shadyside
Pittsburgh
PA
64
Penn State Health – Milton S. Hershey Medical Center
Hershey
PA
76
Penn Medicine Chester County Hospital
West Chester
PA
103
Reading Hospital
Reading
PA
116
St. Luke’s Hospital Bethlehem
Bethlehem
PA
122
Doylestown Hospital
Doylestown
PA
153
Lancaster General Hospital
Lancaster
PA
168
Main Line Health – Lankenau Medical Center
Wynnewood
PA
Top 10 FL Hospitals:
17
Mayo Clinic – Jacksonville
Jacksonville
FL
45
Cleveland Clinic – Florida
Weston
FL
84
Tampa General Hospital
Tampa
FL
146
Sarasota Memorial Hospital
Sarasota
FL
149
St. Joseph’s Hospital – BayCare
Tampa
FL
172
Baptist Health Baptist Hospital
Miami
FL
176
Morton Plant Hospital
Clearwater
FL
179
Baptist Medical Center – Beaches
Jacksonville Beach
FL
183
Adventhealth Orlando
Orlando
FL
215
Cape Canaveral Hospital
Cocoa Beach
FL
NOTE: For patients and their physicians, these rankings and ratings should be seen as just a starting point. While this is helpful information to have, benefit plan participants should also research quality hospitals using transparency tools if these services are available through the health plan or benefits package. For a customized review of your commercial sponsored plan using latest tools and third part-tools please contact us today.
The IRS, yesterday, released the 2024 Health Savings Account (HSA) inflation adjustments. To be eligible to make HSA contributions, an individual must be covered under a high deductible health plan (HDHP) and meet certain other eligibility requirements.
New HSA 2024 limits are as follows:
2024
2023
HSA Annual Contribution Limit
$4,150; $8,300
$3,850 – Single; $7,750 – Family
HDHP Minimum Annual Deductible
$1,600; $3,200
$1,500 – Single; $3,000 – Family
HDHP Out-of-Pocket Maximum
$8,050; $16,100
$7,500 – Single; $15,000 – Family
Age 55+ Catch-Up Provision
$1,000; $2,000
$1,000- Single; $2,000 – Husband/Wife
Age 55 Catch Up Contribution
As in 401k and IRA contributions, you are allowed to contribute extra if you are above a certain age. If you are age 55 or older by the end of the year, you can contribute an additional $1,000 to your HSA. If you are married, and both of you are age 55, each of you can contribute an additional $1,000. A savvy strategy for high-income earners is to invest the money in your HSA for the long haul. Once you’re 65, you can take out tax-free distributions to cover Medicare premiums. If you withdraw money at that point for non-medical uses, you pay the same tax as you would on withdrawals from a pretax 401(k). But you can also take money out tax-free to reimburse yourself for prior years’ out-of-pocket medical expenses if you have the old receipts.
COVId-19 Update:
You can even use an HSA to save on a typical trip to the CVS. Thanks to a tax relief provision tucked in the last Covid-19 stimulus package, you can use the money you stash in an HSA or FSA (more on those later) for over-the-counter medications like Tylenol or Flonase as well as menstrual products like tampons and pads. That reverses Obamacare restrictions on OTC meds requiring a doctor’s prescription for them to be eligible for reimbursement.
HSA/HDHP Market Growth
HSA holders own the assets in the accounts and can build up substantial sums over time. Enrollment in HSA-compatible insurance plans has increased to 10 million earlier this year, from 1 million in March 2005, according to, America’s Health Insurance Plans (AHIP), a trade group.
HSAs were authorized starting in January 2004. Since then, AHIP has conducted a periodic census of health plans participating in the HSA/HDHP market.
The number of people with HSA/HDHP coverage rose to more than 11.4 in January 2011, up from 10.0 million in January 2010, 8.0 million in January 2009, and 6.1 million in January 2008.
30 percent of individuals covered by an HSA plan were in the small-group market, 50 percent were in the large-group market, and the remaining 20 percent were in the individual market.
14% of all workers in the private sector have access to a Health Savings Account acc. to the Bureau of Labor Statistics.
States with the highest levels of HSA/HDHP enrollment were California, Ohio, Florida, Texas, Illinois, and Minnesota.
HSA Advantages:
Opportunity to build savings – Unused money stays in your account from year to year and earns tax-free interest. The HSA also gives you an investment opportunity.
Tax-free contributions and earnings – You don’t pay taxes on contributions or earnings.
Tax-Free Money allowed for non-traditional Medical coverage– As per IRS Publication 502, unused money can be used for dental, vision, Lasik eye surgery, acupuncture, yoga, infertility, etc. Popular Examples
Portability – The funds belong to you, so you keep the funds if you change jobs or retire.
Our overall experience with HSAs has been positive when employer funding is at a minimum 50% using either the HSA or an HRA (Health Reimbursement Account-employer keeps unspent money). Traditional plans trend of higher copays and new in-network deductibles has also led to the popularity of an HSA.
Next Steps
Plan sponsors should update payroll and plan administration systems for the 2023 cost-of-living adjustments and should incorporate the new limits in relevant participant communications, such as open enrollment and communication materials, plan documents, and summary plan descriptions.
Is your HSA compliant? Which pre-tax qualified HSA, FSA, HRA spending card is right for you? Please contact our team at 360PEO (855)667-4621 for immediate answers. Stay tuned for updates as more information gets released. Sign up for the latest news updates.
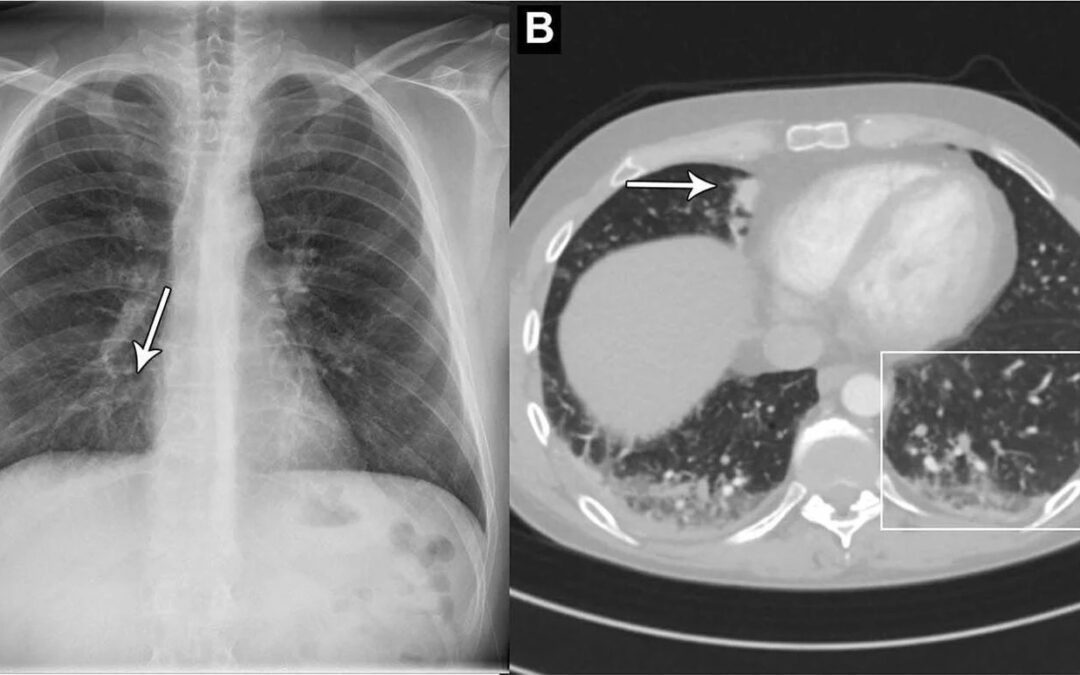
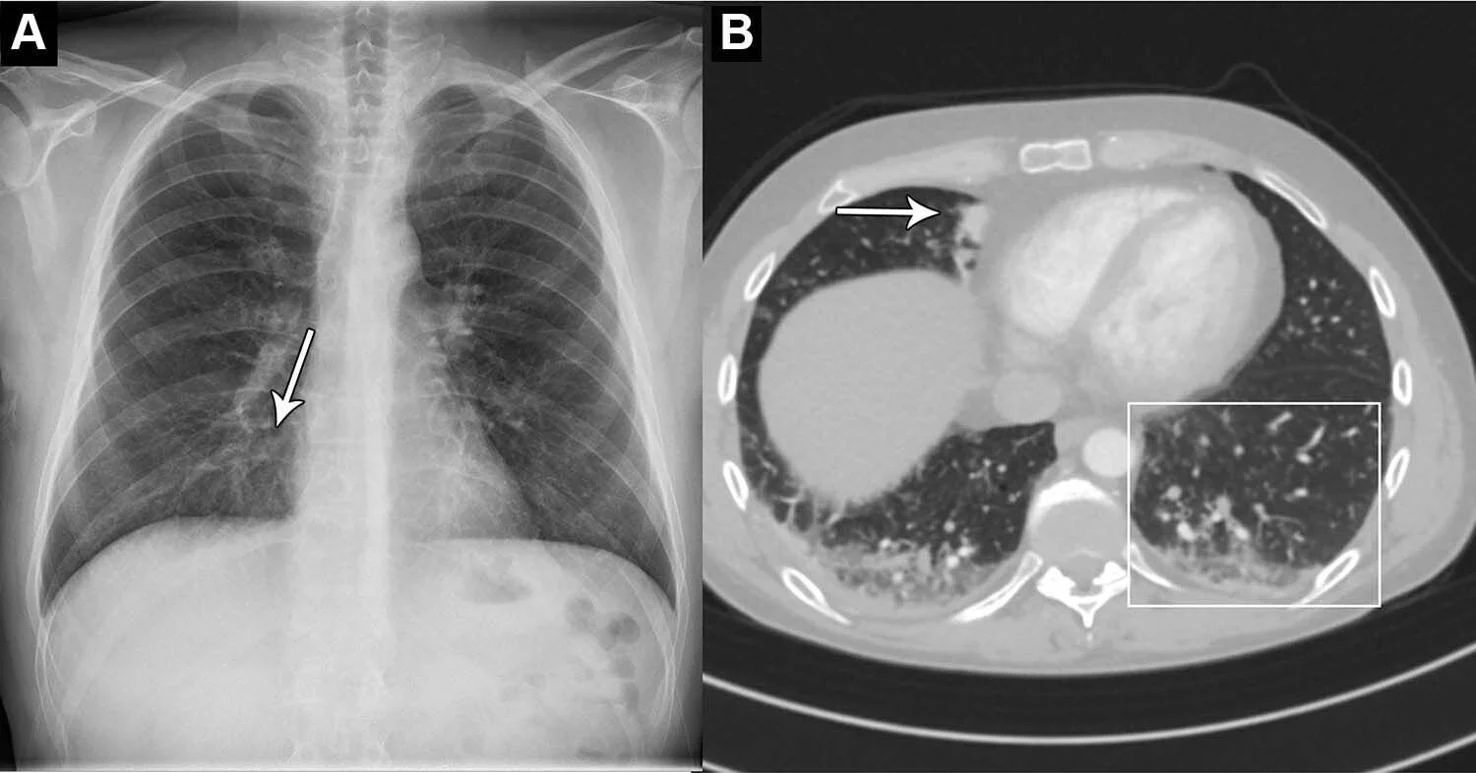
Artificial intelligence can help spot early signs of cancer in chest x-rays, according to a new study.
Scientists found that a state-of-the-art AI tool can identify normal and abnormal chest x-rays in a clinical setting.
Scientists said that an AI tool could accurately differentiate between normal and abnormal chest x-rays. (Photo via SWNS)
Chest X-rays are used to diagnose several conditions to do with the heart and lungs.
An abnormal chest X-ray can be an indication of a range of conditions, including cancer and chronic lung diseases.
Scientists say that an AI tool that can accurately differentiate between normal and abnormal chest X-rays would greatly reduce the heavy workload of radiologists.
Study co-author Dr. Louis Lind Plesner said: “There is an exponentially growing demand for medical imaging, especially cross-sectional such as CT and MRI.
“Meanwhile, there is a global shortage of trained radiologists.
“Artificial intelligence has shown great promise, but should always be thoroughly tested before any implementation.”
Dr. Plesner and his colleagues wanted to determine the reliability of using an AI tool that can identify normal and abnormal chest X-rays.
They used a commercially available AI tool to analyze the chest X-rays of 1,529 patients from four hospitals in Denmark.
Chest X-rays were included from emergency department patients, in-hospital patients and outpatients.
The X-rays were classified by the AI tool as either “high-confidence normal” or “not high-confidence normal,” as in normal and abnormal, respectively.
Two board-certified radiologists were used as the reference standard. A third radiologist was used in cases of disagreements.
Of the 429 chest X-rays that were classified as normal, 120 (28 percent) were also classified by the AI tool as normal. Those X-rays – 7.8 percent of the total – could be potentially safely automated by an AI tool.
The AI tool identified abnormal chest X-rays with a 99.1 percent of sensitivity.
Dr. Plesner, from the Department of Radiology at the Herlev and Gentofte Hospital in Copenhagen, said: “The most surprising finding was just how sensitive this AI tool was for all kinds of chest disease.
“In fact, we could not find a single chest X-ray in our database where the algorithm made a major mistake.
“Furthermore, the AI tool had a sensitivity overall better than the clinical board-certified radiologists.”
He said the AI tool performed particularly well at identifying normal X-rays of the outpatient group at a rate of 11.6 percent.
Dr. Plesener said the findings, published in the journal Radiology, suggest that the AI model would perform especially well in outpatient settings with a high prevalence of normal chest X-rays.
He added: “Chest X-rays are one of the most common imaging examinations performed worldwide.
“Even a small percentage of automatization can lead to saved time for radiologists, which they can prioritize on more complex matters.”
The editorial on the topic praised the potential to take care of 7.8% of all the normal readings for the radiologists, one of the key findings of the study, but suggests that as a labor-saving device, more research is needed to ensure radiologists aren’t putting patients at risk for a mere 7.8% reduction in workload.
The IRS has released the 2023 Flexible Savings Account (FSA) inflation adjustments. These changes will take place for plan years that begin on or after January 1, 2023.
For employers who currently allow the FSA maximum, unless told otherwise, OCA will automatically amend the new FSA maximum to reflect the 2023 increase. OCA will also be providing additional 2023 employee guides/marketing material in the upcoming days. *The limit also applies to limited-purpose FSAs.
On September 1, 2022, Empire BlueCross BlueShield will begin partnering with CareMount Medical, the largest independent, multi-specialty group in New York State, to provide access to affordable care throughout New York City, Westchester, Putnam, Dutchess, Columbia, and Ulster counties.
CareMount will now be part of Empire’s Blue Access and Connection Networks for all Large Group and Small Group members. This will mean greater access to more affordable care throughout Westchester and surrounding markets.
Contact us to learn how Empire can fit your employee’s needs.
Learn more about how we are successfully helping navigate SMB for 25+ years. If you have any questions or would like additional information, please contact us at 855-667-4621 or info@360peo.com.
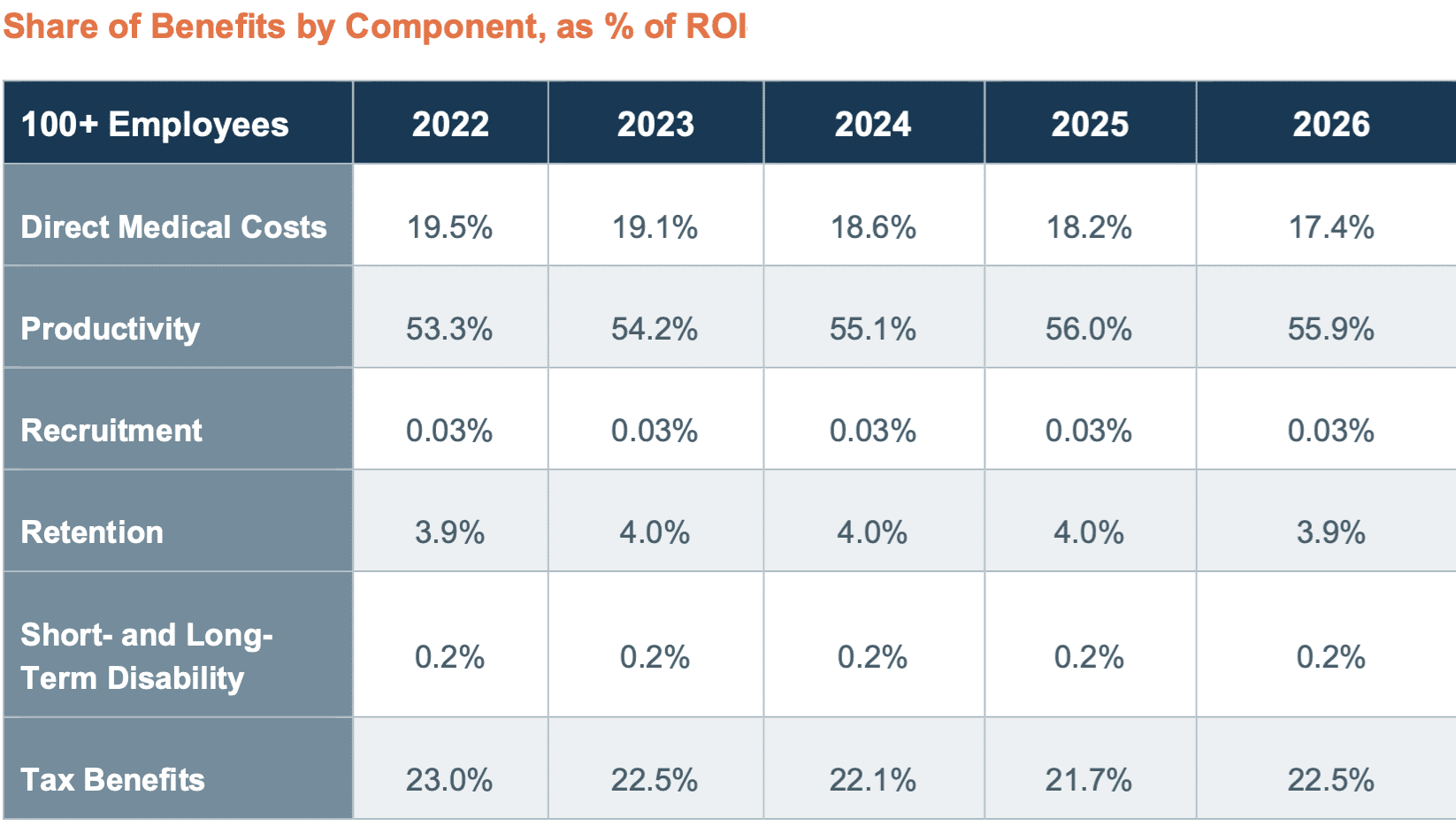
Health insurance is expensive, and we’ve all asked ourselves, “Is it really worth what I am paying?”. For employer-sponsored health insurance, the answer is a resounding YES it is. For every dollar employers spent on health insurance-related costs, they get back $1.47 according to a newstudy from Avalere Health. This figure in fact is expected to grow to 52% by 2026 from 47%.
The U.S. Chamber of Commerce commissioned the Avalere Health employer study that used publicly available data from the Bureau of Labor Statistics and the Congressional Budget Office to estimate the return on investment employer-sponsored health insurance provides employers with 100 or more employees. Improved employee productivity, reduced direct medical costs, and tax benefits were the primary aspects that generated benefits for employer-sponsored health plans. Employers who offered employer-sponsored health coverage and wellness programs had healthier employees and spent less on direct medical costs, Avalare found.
The Numbers
Employee productivity reflects the reductions in absenteeism and lost productivity after receiving employer-sponsored coverage. These productivity increases contributed an estimated $275.6 billion in employer benefits in 2022, or 53.3% of all benefits. By 2026, this is expected to rise to $346.6 billion or 55.9 percent of total ROI.
ROI of some of these key components includes $275.6 billion from improved productivity in 2022 and $346.6 billion in 2026, $101 billion from a reduction in direct medical costs in 2022 and $108 billion in 2026, and $119.2 billion or a 23% ROI from tax benefits in 2022 and $139.7 billion in 2026.
Employer-Sponsored Insurance(ESI) offerings can positively influence prospective employees’ decisions to join firms, reducing employer recruitment and vacancy costs. The study’s model assumes that 9% of individuals decide to accept a certain position based on ESI. The analysis estimates that firms with 100 or more employees derived $141M in employer benefits in 2022, growing to $167M in 2026.
Similarly, ESI positively affects the retention of employees. Avalere’s analysis estimates $20.3B in employer benefits from improved retention in 2022 and $24.3B in 2026.
Conclusion
The study finds that industries where firms generally made greater investments in ESI tended to result in larger ROI. Also, since costs associated with turnover and recruitment are positively associated with wages, Avalere estimates higher ROI in higher-wage industries. On the flip side of that same coin, lower ROI was associated with industries that typically have a lower investment in ESI and wellness programs, lower wages, and lower employee participation in ESI and wellness programs.
The full report including the methodology can be found here.
For more information on how Employer-Sponsored Insurance and a PEO can make difference for your small business please contact us at info@360peo.com or 855-667-4621.
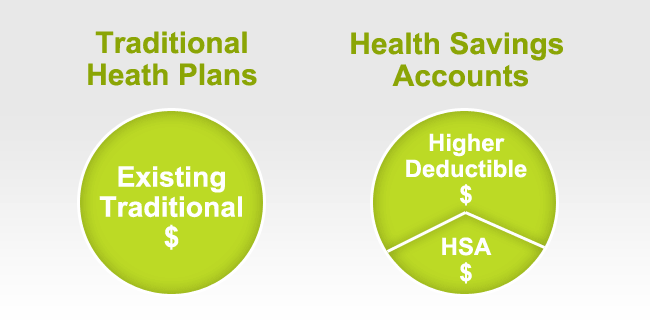
How High Deductible Health Plans Can Set Employees Up for Financial Success
Overview
A common fear among employees can be that High Deductible Health Plans (HDHPs) expose them to too much risk. However, this misconception misses the near-certain long-term losses that come with not choosing a HDHP that includes an HSA. What employees are often missing is a full knowledge of the long-term financial impacts and risks associated with enrolling in an HDHP paired with HSA savings strategy, compared to a more traditional, low deductible PPO option. Employer contributions to HSAs can also set employees up for financial success and retirement readiness.
More Info
Join this complimentary webcast to discover how HSA-eligible plans are better for employees in the long run and can help improve their financial health. Topics discussed will include:
The short term risks that scare employees away from an HSA plan
The long term benefits that make HSAs a no-brainer
Ways to overcome employees’ apprehension towards HSAs to get them to enroll and contribute
And more…
Date: Wednesday, June 15 2022
Time: 2:00 p.m. ET
Cost: Complimentary
Day(s)
:
Hour(s)
:
Minute(s)
:
Second(s)
Samuel Kina, Ph.D. | Chief Analytics Officer | Picwell, Inc.
Bio
Samuel Kina, Ph.D. is the Chief Analytics Officer at Picwell, Inc. where he has led the company’s work in economic and predictive modeling since 2014, shortly after the company was founded. He has a wide range of experience in health policy and economics in the public, private, and non-profit sectors. He has advised several state and private health insurance exchanges, and he has provided economic and strategic support to several pharmaceutical manufacturers, health insurance companies, regulatory agencies, and Congress in matters related to health policy, intellectual property, antitrust regulation and FDA regulation and drug approval. Sam has taught courses in statistics, economics, and health policy, and his research has focused on the economics of the health insurance and pharmaceutical industries.
Prior to joining Picwell, he held positions at the Analysis Group, Congressional Budget Office, and the Alliance for Health Reform. Sam has a BA in Public Policy Analysis and Economics from Pomona College and a Ph.D. in Health Policy and Economics from Harvard University.
REGISTER NOW! (Not able to attend? We recommend you STILL REGISTER – you will receive an email with how to access the recording of the event)
Join Our Newsletter
Subscribe for news & resources about scaling your business
The IRS has released the 2023 Health Savings Account (HSA) inflation adjustments. To be eligible to make HSA contributions, an individual must be covered under a high deductible health plan (HDHP) and meet certain other eligibility requirements.
New HSA 2023 limits are as follows:
2023
2022
HSA Annual Contribution Limit
$3,850; $7,750
$3,650 – Single; $7,300 – Family
HDHP Minimum Annual Deductible
$1,500; $3,000
$1,400 – Single; $2,800 – Family
HDHP Out-of-Pocket Maximum
$7,500; $15,000
$7,050 – Single; $14,100 – Family
Age 55+ Catch-Up Provision
$1,000; $2,000
$1,000- Single; $2,000 – Husband/Wife
Age 55 Catch Up Contribution
As in 401k and IRA contributions, you are allowed to contribute extra if you are above a certain age. If you are age 55 or older by the end of the year, you can contribute an additional $1,000 to your HSA. If you are married, and both of you are age 55, each of you can contribute an additional $1,000. A savvy strategy for high-income earners is to invest the money in your HSA for the long haul. Once you’re 65, you can take out tax-free distributions to cover Medicare premiums. If you withdraw money at that point for non-medical uses, you pay the same tax as you would on withdrawals from a pretax 401(k). But you can also take money out tax-free to reimburse yourself for prior years’ out-of-pocket medical expenses if you have the old receipts.
COVId-19 Update:
You can even use an HSA to save on a typical trip to the CVS. Thanks to a tax relief provision tucked in the last Covid-19 stimulus package, you can use the money you stash in an HSA or FSA (more on those later) for over-the-counter medications like Tylenol or Flonase as well as menstrual products like tampons and pads. That reverses Obamacare restrictions on OTC meds requiring a doctor’s prescription for them to be eligible for reimbursement.
HSA/HDHP Market Growth
HSA holders own the assets in the accounts and can build up substantial sums over time. Enrollment in HSA-compatible insurance plans has increased to 10 million earlier this year, from 1 million in March 2005, according to, America’s Health Insurance Plans (AHIP), a trade group.
HSAs were authorized starting in January 2004. Since then, AHIP has conducted a periodic census of health plans participating in the HSA/HDHP market.
The number of people with HSA/HDHP coverage rose to more than 11.4 in January 2011, up from 10.0 million in January 2010, 8.0 million in January 2009, and 6.1 million in January 2008.
30 percent of individuals covered by an HSA plan were in the small group market, 50 percent were in the large-group market, and the remaining 20 percent were in the individual market.
14% of all workers in the private sector have access to a Health Savings Account acc. to the Bureau of Labor Statistics.
States with the highest levels of HSA/HDHP enrollment were California, Ohio, Florida, Texas, Illinois, and Minnesota.
HSA Advantages:
Opportunity to build savings – Unused money stays in your account from year to year and earns tax-free interest. The HSA also gives you an investment opportunity.
Tax-free contributions and earnings – You don’t pay taxes on contributions or earnings.
Tax-Free Money allowed for non-traditional Medical coverage– As per IRS Publication 502, unused money can be used for dental, vision, Lasik eye surgery, acupuncture, yoga, infertility, etc. Popular Examples
Portability – The funds belong to you, so you keep the funds if you change jobs or retire.
Our overall experience with HSAs has been positive when employer funding is at a minimum 50% using either the HSA or an HRA (Health Reimbursement Account-employer keeps unspent money). Traditional plans trend of higher copays and new in-network deductibles has also led to the popularity of an HSA.
Next Steps
Plan sponsors should update payroll and plan administration systems for the 2022 cost-of-living adjustments and should incorporate the new limits in relevant participant communications, such as open enrollment and communication materials, plan documents, and summary plan descriptions.
Is your HSA compliant? Which pre-tax qualified HSA, FSA, HRA spending card is right for you? Please contact our team at 360PEO (855)667-4621 for immediate answers. Stay tuned for updates as more information gets released. Sign up for the latest news updates.
Effective April 1, 2022, high-deductible health plans can once again offer first-dollar coverage for Telehealth and other remote services without making participants ineligible for health savings account (“HSA”) contributions. The relief runs only through the end of 2022. This relief allows individuals with High Deductible Health Plans (“HDHPs”) to receive free telehealth services prior to the satisfaction of their minimum deductible and remain eligible to make Health Savings Account (“HSA”) contributions.
Background
Individuals may contribute to an HSA if they are covered by a qualifying HDHP and do not have other disqualifying coverage. Generally, telehealth or other remote health care services are considered other health care coverage that, if provided before satisfaction of the required deductible, may be disqualifying for purposes of contributing to an HSA.
The Coronavirus Aid, Relief, and Economic Security Act (the “CARES Act”) were signed into law on March 27, 2020. Among other things, the CARES Act offered temporary relief related to telehealth and other remote care services when offered with an HDHP and HSA. Specifically, for plan years beginning on or before December 31, 2021, telehealth and other remote care services could be offered before satisfaction of the deductible without jeopardizing an individual’s eligibility to contribute to an HSA.
Employer Action
Employers offering HDHPs with HSAs should consider whether to re-implement (or continue) free telehealth as part of a benefit offering. Employers with calendar year plans may
have already re-introduced a cost associated with telehealth for HDHP/HSA participants once the CARES Act relief expired and should consider whether to waive those costs again given the temporary nature of this relief. Additionally, employers with non-calendar year plans should consider the administrative and communication burdens that may be imposed by providing relief that may expire prior to the end of the current plan year.
It is important that employers review these changes with their carriers, Third Party Administrators and telehealth vendors to understand their approach and communicate any changes with participants.
Learn more about how we are successfully helping navigate SMB for 20+ years. If you have any questions or would like additional information, please contact us at 855-667-4621 or info@360peo.com.
We already love Professional Employer Organization (PEO)– our clients do too. Today we’re counting down our top 5 reasons why we love PEO:
1.National Capabilities:
It ensures your compliance with local and federal laws, even if your business has locations in different states. Access to a national provider healthcare plan, not single state carriers
2. Liability Protections:
Some liability moves to the PEO service instead of your company.
3. It saves you money on HR staff.
Being part of a PEO gives you a clear cut idea of what your costs are going to be year in and year out. The PEOs work tirelessly to keep their insurance renewals down, so their clients won’t leave. Every year they work with the insurance carriers to introduce new plans and ways to reduce the costs of insurance to their clients. This gives you the ability to forecast and know precisely what your costs will be.
4. Technologies:
Online HR resources for self service issues Ability for employees to make personal changes on their own, online. Ability to track PTO (paid-time off).
5. One Vendor:
It streamlines HR tasks like payroll, taxes, employee benefits, worker’s compensation, 401K and HR administrative tasks.
Our PEO Quoting Tool ensures that we have first-hand insight as to what the small business owner needs to be successful. Click below for quote.
Free At-Home COVID-19 Test available via USPS. On Jan. 18, every home in the United States can order up to four free COVID-19 tests. January 19, Americans will be able to order free at-home rapid COVID tests from the government at COVIDTests.gov.
The federal guidance requires commercial insurers and group health plans (both fully insured and self-insured) to reimburse consumers for the cost of Over-the-Counter (OTC) COVID-19 diagnostic tests, with or without an order or clinical assessment by a healthcare provider.
Types of COVID Tests:
Antigen tests, which test for an active infection by detecting specific virus proteins. Most at-home tests and “rapid tests” performed by healthcare providers fall in this category.
Molecular tests, which test for an active infection by amplifying genetic material from the virus. These are considered the “gold standard” for diagnosing COVID, as they are generally more accurate than antigen tests. The most familiar test from this category is the polymerase chain reaction (or PCR) test, which requires lab processing.
Antibody tests, which are blood tests that determine if the body has had an immune response to the virus. These tests are not used for diagnosing an active infection.
How Will this work with your Insurer?
Consistent with the guidance Insurers will utilize existing member claims submission procedures to provide benefits without cost-share for OTC COVID-19 tests that members purchase, either online or through other retailers. In addition to the member demographic information that is normally filed with member-submitted claims, the members will be required to certify that the test was purchased for personal use and not for employment purposes.
Customers may receive reimbursement for up to 8 COVID-19 OTC tests per covered individual per calendar month without a health care provider prescription or individualized clinical assessment. For a family of four covered individuals, that equates to 32 tests per month.
Members with Empire Blue Cross, for example, will utilize A.I. apps such as Sydney App or online. Separately, Insurers such as UnitedHealthcare will initially offer for at-home COVID-19 tests are Walmart Pharmacy and Rite Aid Pharmacy. When using Walmart or Rite-Aid there will be no up-front cost and you will not have to submit a form for reimbursement. Note, you may be required to go to the pharmacy counter to obtain the test kits at no cost.
If you’re interested in hearing more about the advantages of partnering with a PEO, we’d love to talk to you. Fill out the form below or email info@medicalsolutionscorp.com for a FREE Consultation Today!
The information provided on this website is intended for informational purposes only. Millennium Medical Solutions Corp. does not offer legal or medical guidance. Those with legal or medical questions should seek appropriate assistance from a licensed professional. Stay up to date by signing up for Newsletter and Coronavirus Dashboard below.
You can get ahead of cold and flu season by embracing a few habits that can help support a healthy immune system.
Plus, boosting your natural immunity doesn’t have to be time-consuming or expensive.
You may be doing some of these things already. If not, take baby steps to build new habits, because trying to do too much too soon may lead to frustration.
What steps can you take to fit these five tips into your life?
1. Get a good night’s rest.
Like stress, sleep deprivation can reduce the effectiveness of your immune system and lead to a longer recovery time if you do get sick.
Practice good sleep habits like putting away your devices before bed and creating a wind-down routine to help you relax.
2. Watch your stress levels.
Stress can weaken your immune system, making it harder to fight off a cold or the flu. Try practicing stress-reduction techniques such as daily meditation or breathing exercises.
3. Keep your hands clean.
Wash your hands often, especially when entering or leaving public places or touching surfaces. Cleaning your hands with soap and water for at least 20 seconds can be the best way to remove germs. When that’s not possible, use a hand sanitizer with at least 60% alcohol.
4. Stay active.
Exercise can help alleviate stress and support your immune system — and physical activity doesn’t have to be intense to make a difference. To get started, you can try taking a daily walk or practicing gentle yoga poses.
5. Focus more on nutrition.
A healthy diet supports a healthy immune system. In addition to the supplements, you may already take, try to eat foods rich in vitamins and minerals, such as:
Citrus fruits
Spinach
Green tea
Shellfish
Cleveland Clinic: We’re now several months into the coronavirus pandemic, and we’re also fast-approaching peak season for yet another viral illness: influenza. Infectious disease specialist Kristin Englund, MD, explains the differences between COVID-19 and the flu, and shares steps we can all take to help us stay healthy this flu season.
For information about transparency providers and new tech tools contact us at info@medicalsolutionscorp.com or (855)667-4621.
sCMS and OSHA released interim final rules this week detailing the implementation of national vaccine requirements established by President Biden’s executive order in September.Yesterday, the Department of Labor released an unpublished version of the OSHA Emergency Temporary Standard (ETS).
The ETS is effective immediately and will cover 2/3rds of private employers. The OSHA ETS puts into effect the Biden Executive Order mandating all private employers with 100 or more employees ensure their employees are vaccinated against COVID-19, or submit negative weekly tests.
KEY Summary:
Covered Employers
Private employers with 100 or more employees enterprise-wide (across US locations) at the time these rules become effective
Independent contractors not included
Special franchisee, construction and staffing agency rules
Companies who grow will move into the covered group
State/local governments, including schools
Only state/local ordinances/laws that are not conflicting will have effect (i.e., if the state law prohibits vaccine mandates, OSHA ETS will supersede state law. OSHA ETS will be mandated.)
States with state OSHA plans may adopt these federal rules or similar rules. Some states are threatened with removal of state plan authority for failure to comply with laws as stringent as federal (e.g., UT & AZ)
Compliance Deadline
Within 30 days of publication (December 5)
Testing requirements within 60 days (January 4)
Mandate
Determine vaccination status of each employee
Obtain acceptable proof –
Maintain records/roster
Unvaccinated must test negative weekly if worker in workplace at least once a week or within 7 days before returning to work if worker is away from workplace a week or longer
Must wear face covering indoors or in occupied vehicle for work
Employer not required to pay for testing unless required by law or collective bargaining agreement
Employer not required to pay for face coverings
Notice
Employee must promptly notify of positive COVID test or receive diagnosis
Employer must remove employee from workplace, regardless of vaccination status
May not return to work until meeting criteria
Must provide paid time off for vaccination and recovery from side effects
In conclusion, employers subject to the ETS must determine whether they will take a vaccine-only or combined vaccine and testing/face covering approach to compliance and must develop the required written policies and communicate those policies to employees so they have ample time to receive their COVID-19 vaccines. Employers should work with legal counsel to develop their written policies and to address any reasonable accommodation requests received by employees.
If needing employment law assistance in implementing these new rules, contact your World Insurance Associates representative so that they can connect you a Jackson Lewis P.C. council in order to receive the WIA arrangement. For our PEO clients, please speak with in-house council and HR.
The information provided in this alert is not, is not intended to be, and shall not be construed to be, either the provision of legal advice or an offer to provide legal services, nor does it necessarily reflect the opinions of the agency, our lawyers, or our clients. This is not legal advice. Rather, the content is intended as a general overview of the subject matter covered.
Good news Bronx/Westchester. Oxford and Montefiore Health System announced moments ago that they have reached an agreement effective December 1, 2021 for UnitedHealthcare and Oxford employer-sponsored plans, as well as UnitedHealthcare’s Medicare Dual Special Needs Plan.
This resolves a split since Jan 1, 2021 which affected a significant percentage of local residents as both companies have a critical size of the market. Westchester and Bronx populations total nearly 2.5 million people. While this contract is resolved with titanic and a few Hospital Systems and Insurers left in the market we expect to see this trend to continue.
See below the official press release.
UnitedHealthcare and Montefiore Health System Renew Relationship
UnitedHealthcare and Montefiore Health System have reached a multi-year agreement that restores access to Montefiore’s hospitals and physicians for people enrolled in UnitedHealthcare and Oxford employer-sponsored plans as well as UnitedHealthcare’s Medicare Dual Special Needs Plan, effective Dec. 1, 2021.
We recognize that the care Montefiore provides is not only important but also personal to our members and we also know the negotiations process may have been difficult for them. Our top priority throughout this process was ensuring the people and employers we’re honored to serve in New York have access to quality, more affordable health care, and this new agreement helps accomplish that goal.
We thank our members and customers for their support and patience throughout this process. We are honored to continue supporting the more than 3.7 million individuals across New York who depend on us for access to quality and affordable health care.
Montefiore Hospitals & Health System
Facility Name
County
Montefiore Hospital (Moses Campus)
Bronx
Children’s Hospital at Montefiore
Bronx
Garnet Health MedJack D. Weiler Hospital (Einstein Campus)ical Center
Bronx
Montefiore Wakefield Hospital (Wakefield Campus)
Bronx
Burke Rehabilitation Hospital
Westchester
Montefiore Mount Vernon Hospital
Westchester
Montefiore New Rochelle Hospital
Westchester
Montefiore Nyack Hospital
Rockland
Montefiore St Luke’s Cornwall Hospital
Orange
White Plains Hospital
Bronx
Montefiore Hutchinson Campus
Bronx
Montefiore Medical Group
Westchester
Montefiore Medical Specialists of Westchester
Westchester
Neighboring Hospitals
Facility Name
County
Bon Secours Community Hospital BronxCare Hospital Center Garnet Health Medical Center Good Samaritan Hospital of Suffern New York Presbyterian Hudson Valley Hospital New York Presbyterian Lawrence Hospital NYC Health + Hospitals Jacobi NYC Health + Hospitals Lincoln NYC Health + Hospitals North Central Bronx St. Anthony Community Hospital St. Barnabas Hospital St. John’s Riverside Hospital Westchester Medical Center
Medicare Supplemental Plan F phased out for newly Medicare eligible? With the new 2022 open enrollment changes, it’s time to get the facts. Considering making changes to your coverage this fall or just want to learn more about this enrollment period?
During the Medicare open enrollment period – which runs from October 15 through December 7 – you can make a variety of changes (none of which involve medical underwriting):
Switch from Medicare Advantage toOriginal Medicareor vice versa.
Switch from one Medicare Advantage plan to another.
Switch from onePart D prescription planto another.
Join a Medicare Part D plan.
Drop your Part D coverage altogether.
1. Medicare Supplement Plans F and C are still available
While the Centers for Medicare and Medicaid (CMS) will no longer allow newly eligible Medicare beneficiaries to enroll in Medigap plans F and C, these plans aren’t disappearing completely. If you become eligible for Medicare before January 1, 2021 (and that’s everyone who can use the 2021 fall Medicare Open Enrollment Period), you can apply for these plans now and in the future—even if you aren’t already enrolled in Medigap.
If you become eligible for Medicare on or after January 1, 2020, you won’t be able to enroll in Plans F or C now or in the future.
2. The Part D ‘donut hole’ will close
In 2022, you’ll enter the donut hole when your spending + your plan’s spending reaches $4,430. And you leave the donut hole — and enter the catastrophic coverage level — when your spending + manufacturer discounts reach $7,050. Both of these amounts are higher than they were in 2021, and generally increase each year. Learn more about Part D.
3. Changes in Medicare Advantage and Part D plans
Every year, insurers make small changes to their Medicare Advantage and Part D plans. Typically, these changes include changes in premiums, deductibles, and other costs. Keep in mind, the Medicare program may not finalize these changes until right before fall Open Enrollment.
See the latest Medicare premiums and deductibles now or come back in October. We’ll share finalized changes as soon as they become available.
Refresh your general Medicare knowledge
While the Medicare program changes a bit each year, much of it stays the same. It never hurts to refresh your Medicare knowledge. We recommend starting with an Overview of Medicare. This Medicare Glossary could come in handy, too, as you read through insurance documents. See
Medicare Part B premiums increased this year by about 2.7% or $4 per month and high-income surcharges also rose modestly in 2021. For 2022 the Standard Part B premiums are projected to be $158.50/month from $148.50/month in 2021 or a 6.7% increase.
The wealthiest senior couples will be paying more than $12,000 a year in Medicare Part B premiums. Part B (the base and the surcharge) covers doctors’ and outpatient services. Medicare Part B Income-Related Monthly Adjustment Amounts.
5. Part B deductible also increased for 2021, and will increase again in 2022
Medicare B also has a deductible, which increased to$203 in 2021, up from$198 in 2020. For 2022, the Part B deductible isprojected to be $217. The Medicare Part B deductible only has to be paid once per year, unlike the Part A deductible, which has to be paid once perbenefit period.
Do you have to renew your plan?
If you’re happy with your Medicare coverage, there’s no need to do anything during Medicare Open Enrollment. Provided your current plan is available next year, your coverage will auto-renew.
Although you could let Open Enrollment pass right on by without having to lift a finger, we recommend doing two things this fall to optimize your Medicare coverage.
1. Read Medicare Mailers
If your plan is discontinued next year, you’ll receive a notice in the mail. If you miss this notice and fail to enroll in other coverage, you could lose your coverage.
If your plan continues in the following year, your insurer will send you an Annual Notice of Change (ANOC). Look over your ANOC carefully to make sure your plan will still meet your needs next year. If not, its time to consider other options.
No matter how you feel about your current plan, it’s usually a good idea to do a little shopping around during Open Enrollment. Since plans and premiums change annually, options that fit your situation even better than your current coverage could pop up. But if you don’t check, you’ll never know.
Know These Dates
OCT 15 - DEC 7
OPEN ENROLLMENT PERIOD for Medicare Advanatage and Medicare Part D Prescription Drug coverage. All individuals with Medicare can change their Medicare health plan and prescription drug coevrage for the next year.
JAN 1 - FEB 14
MEDICARE ADVANTAGE DISENROLLMENT PERIOD. Those with MA plans (Part C) can leave the plan and switch to original Medicare.
JAN 1 - DEC 31
MEDICARE SUPPLEMENT (Medigap) plans can be purchaded year-round but may require answering health questions to determine eligibility.
Total Number of Million Medicare Beneficiaries. Source: Kaiser Family Foundation
2020
2018
2017
2015
Click Above
Plan Comparison Tool
Enroll Online
tings.
Call
Call to speak to a licensed sales agent 855-667-4621 (TTY 711)
Cybersecurity Awareness Month is intended to raise employee awareness in every way possible.
It’s never been more important for cybersecurity to be top of mind for all of us. We are all connected to the internet both professionally and personally, therefore, we are all exposed to the bad guys. To that end, it’s important that we know how to prevent cybersecurity attacks and what it means to do our part and be Cyber Smart.
Stats
The U.S government allocated an estimated $18.78 billion for cybersecurity spending in 2021.
Damage related to cybercrime is projected to hit $10.5 trillion annually by 2025.
64% of Americans have never checked to see if they were personally affected by a data breach.
16% of healthcare providers reporting having “fully functional” security programs.
In April 2020, Google blocked 18 million daily malware and phishing emails related to COVID.
89% of healthcare organizations had patient data lost or stolen in the past two years.
Google has registered 2,145,013 phishing sites as of January 17, 2021. This is up from 1,690,000 on January 19, 2020.
20% of organizations said they faced a security breach as a result of a remote worker.
Norton LifeLock Advantage
We are excited to announce a new partnership with NortonLifeLock for SMB with two or more employees, provide a cybersecurity offering to their employees. As a global leader in consumer cyber safety, NortonLifeLock has built a comprehensive and easy-to-use integrated portfolio that prevents, detects, and responds to cyber threats and cybercriminals in today’s digital world. With over four decades of experience in cybersecurity and identity theft protection, NortonLifeLock helps people live their digital lives safely and has earned the trust of over 80 million users in more than 150 countries. Learn more in this shortvideo.
Everyday actions including online shopping, banking, and even simply browsing the internet can expose your clients’ personal information and make them more vulnerable to cybercriminals. Since cybercrime hasevolved, NortonLifeLock has evolved as well. LifeLock, a leader in identity theft protection, and Norton, a pioneer in consumer cybersecurity, are now one company. Their innovative employee benefit plans will helpprotect an employee’s identity, personal information, and connected devices against the myriad of threats they may face in their digitally connected homes, workplaces, and when using public Wi-Fi.
If you see something say something. The bad guys only have to get it right once, we need to get it right every time!
Our WIA Cyber Team and helpdesk are here to help our clients. . Take a company audit, your preparedness is your responsibility.
A little-known requirement but most important under Affordable Care Act (ACA) is for Health Insurers must waive their minimum employer-contribution and employee-participation rules once a year. ACA requires a one-month Special Open Enrollment Window for January 1st coverage.
The special open enrollment period occurs November 15th through December 15th of each year, allowing eligible small group employers to enroll for coverage effective January 1st of the following year.
Background
The ACA has a section in it called the “guaranteed issuance of coverage in the individual and group market.” It stipulates that “each health insurer that offers health insurance coverage in the individual or group market in the state must accept every employer and individual in the state that applies for such coverage.” The section also states that this guaranteed issuance of coverage can only be offered during (special) open enrollment periods, and that plans can only be offered to applicants that live in, work in, or reside in the plans’ service area(s).
Participation and Contribution Requirements
In many states (including California and Nevada), carriers can decline to issue group health coverage if fewer than 70% of employees elect to enroll in coverage. Some carriers may have even tighter participation requirements.
Generally speaking, employees with other coverage (Medicare, other group coverage, individual coverage through the Exchange, etc.) are removed from the participation requirement calculation – though it varies by insurance carrier.
Furthermore, employer contribution rules require employers to contribute a certain percentage of premium costs for all employees in order to attain group health coverage. Some businesses struggle to meet these contribution requirements for a variety of financial reasons.
Problem Solved: Special Open Enrollment Period
Many employers want to offer coverage to their employees, but are denied because they struggle to meet participation and/or contribution requirements. Employers cannot force employees to enroll in coverage unless the employer pays for 100% of the employees’ premiums, which many employers cannot afford. Even with moderate to generous employer contributions, many employers still find young and lower-income employees waiving coverage. This was even more evident in 2019 with the ACA’s federal Individual Mandate non-compliance penalty reduced to $0.00.
The U.S. Department of Health & Human Services provides final guidance on this in regulation 147.104(b)(1): “In the case of health insurance coverage offered in the small group market, a health insurance issuer may limit the availability of coverage to an annual enrollment period that begins November 15 and extends through December 15 of each year in the case of a plan sponsor that is unable to comply with a material plan provision relating to employer contribution or group participation rules.”
If your employer groups are struggling with participation and/or contribution, the Special Open Enrollment Window is the time to enroll them in coverage.
This Compliance Overview is not intended to be exhaustive nor should any discussion or opinions be construed as legal advice. Readers should contact legal counsel for legal advice.
In preparation for open enrollment, Employers should review their plan documents in light of changes for the plan year beginning Jan 1, 2021. Below is an Employer 2 Open Enrollment Checklist including some administrative items to prepare for in 2020.
Health plan sponsors should also confirm that their open enrollment materials contain certain required participant notices, when applicable—for example, the summary of benefits and coverage (SBC). There are also some participant notices that must be provided annually or upon initial enrollment. To minimize costs and streamline administration, employers should consider including these notices in their open enrollment materials.
PLAN DESIGN CHANGES
Out-of-pocket Maximum
Effective for plan years beginning on or after Jan. 1, 2014, non-grandfathered health plans are subject to limits on cost-sharing for essential health benefits (EHB). The ACA’s out-of-pocket maximum applies to all non-grandfathered group health plans, including self-insured health plans and insured plans.
$8,700 for self-only coverage and $17,400 for family coverage out-of-pocket maximum.
$7,050 for self-only coverage and $14,100 for family coverage HSA Maximum. For 2021 plan years, the out-of-pocket maximum limit for HDHPs is $7,000 for self-only coverage and $14,000 for family coverage.
Preventive Care Benefits
The ACA requires non-grandfathered health plans to cover certain preventive health services without imposing cost-sharing requirements (that is, deductibles, copayments or coinsurance) for the services. Health plans are required to adjust their first-dollar coverage of preventive care services based on the latest preventive care recommendations. If you have a non-grandfathered plan, you should confirm that your plan covers the latest recommended preventive care services without imposing any cost-sharing.
The ACA imposes a dollar limit on employees’ salary reduction contributions to a health flexible spending account (FSA) offered under a cafeteria plan. An employer may impose its own dollar limit on employees’ salary reduction contributions to a health FSA, as long as the employer’s limit does not exceed the ACA’s maximum limit in effect for the plan year.
The ACA set the health FSA contribution limit at $2,500. For years after 2013, the dollar limit is indexed for cost-of-living adjustments. For 2022 plan years, the health FSA limit is $2,850. The DFSA Rollover Maximum is $570.
Communicate the health FSA limit to employees as part of the open enrollment process.
HDHP and HSA Limits for 2022
If you offer an HDHP to your employees that is compatible with an HSA, you should confirm that the HDHP’s minimum deductible and out-of-pocket maximum comply with the 2020 limits. The IRS limits for HSA contributions and HDHP cost-sharing increase for 2022. The HSA contribution limits will increase effective Jan. 1, 2022, while the HDHP limits will increase effective for plan years beginning on or after Jan. 1, 2022.
Check whether your HDHP’s cost-sharing limits need to be adjusted for the 2022 limits.
If you communicate the HSA contribution limits to employees as part of the enrollment process, these enrollment materials should be updated to reflect the increased limits that apply for 2022.
The following table contains the HDHP and HSA limits for 2022 as compared to 2021. It also includes the catch-up contribution limit that applies to HSA-eligible individuals who are age 55 or older, which is not adjusted for inflation and stays the same from year to year.
Type of Limit
2021
2022
Change
HSA Contribution Limit
Self-only
$3,600
$3,650
Up $50
Family
$7,200
$7,300
Up $100
HSA Catch-up Contributions (not subject to adjustment for inflation)
Age 55 or older
$1,000
$1,000
No change
HDHP Minimum Deductible
Self-only
$1,400
$1,400
No change
Family
$2,800
$2,800
No change
HDHP Maximum Out-of-pocket Expense Limit (deductibles, copayments and other amounts, but not premiums)
Self-only
$7,000
$7,050
Up $50
Family
$14,000
$14,100
Up $100
ACA EMPLOYER MANDATE AND OTHER REQUIREMENTS
Applicable Large Employer Status (ALE)
Under the ACA’s employer penalty rules, applicable large employers (ALEs) that do not offer health coverage to their full-time employees (and dependent children) that is affordable and provides minimum value will be subject to penalties if any full-time employee receives a government subsidy for health coverage through an Exchange.
To qualify as an ALE, an employer must employ, on average, at least 50 full-time employees, including full-time equivalent employees (FTEs), on business days during the preceding calendar year. All employers that employ at least 50 full-time employees, including FTEs, are subject to the ACA’s pay or play rules.
Determine your ALE status for 2022
Calculate the number of full-time employees for all 12 calendar months of 2020. A full-time employee is an employee who is employed on average for at least 30 hours of service per week.
Calculate the number of FTEs for all 12 calendar months of 2021 by calculating the aggregate number of hours of service (but not more than 120 hours of service for any employee) for all employees who were not full-time employees for that month and dividing the total hours of service by 120.
Add the number of full-time employees and FTEs (including fractions) calculated above for all 12 calendar months of 2021.
Add up the monthly numbers from the preceding step and divide the sum by 12. Disregard fractions.
If your result is 50 or more, you are likely an ALE for 2022.
Identify Full-time Employees
All full-time employees must be offered affordable minimum value coverage. A full-time employee is an employee who was employed on average at least 30 hours of service per week. The final regulations generally treat 130 hours of service in a calendar month as the monthly equivalent of 30 hours of service per week. The IRS has provided two methods for determining full-time employee status—the monthly measurement method and the look-back measurement method.
Determine which method you are going to use to determine full-time status
The monthly measurement method involves a month-to-month analysis where full-time employees are identified based on their hours of service for each month. This method is not based on averaging hours of service over a prior measurement method. Month-to-month measuring may cause practical difficulties for employers, particularly if there are employees with varying hours or employment schedules, and could result in employees moving in and out of employer coverage on a monthly
The look-back measurement method allows an employer to determine full-time status based on average hours worked by an employee in a prior period. This method involves a measurement period for counting/averaging hours of service, an administrative period that allows time for enrollment and disenrollment, and a stability period when coverage may need to be provided, depending on an employee’s average hours of service during the measurement
Audit FTEs for FMLA Compliance
Audit your FTEs to determine if you have reached or exceeded 50 employees and are required to comply with the Family Medical Leave Act (FMLA) in 2022. Employers covered by the FMLA are obligated to provide their employees with certain important FMLA notices, so both employees and the employer have a shared understanding of the terms of the FMLA leave. Note that FMLA compliance requirements are different from ACA compliance.
Offer of Coverage
An ALE may be liable for a penalty under the pay or play rules if it does not offer coverage to “substantially all” (95%) full-time employees (and dependents) and any one of its full-time employees receives a premium tax credit or cost-sharing reduction for coverage purchased through an Exchange. For employees who are offered health coverage that is affordable and provides minimum value are generally not eligible for these Exchange subsidies. The IRS lowered the 2022 employer health plan affordability threshold, or cost-sharing limit, to 9.61% of an employee’s income. The threshold in 2021 was 9.83%.
Offer minimum essential coverage to all full-time employees
Ensure that at least one of those plans provides minimum value (60% actuarial value)
Ensure that the minimum value plan offered is affordable to all full-time employees by ensuring that the employee contribution for the lowest cost single minimum value plan does not exceed 78% of an employee’s earnings based on the employee’s W-2 wages, the employee’s rate of pay, or the federal poverty level for a single individual.
Reporting of Coverage
The ACA requires ALEs to report information to the IRS and to employees regarding the employer-sponsored health coverage on Form 1095-C. The IRS will use the information that ALEs report to verify employer-sponsored coverage and to administer the employer shared responsibility provisions (Code Section 6056).
In addition, the ACA requires every health insurance issuer, sponsor of a self-insured health plan, a government agency that administers government-sponsored health insurance programs and any other entity that provides minimum essential coverage (MEC) to file an annual return with the IRS and individuals reporting information for each individual who is provided with this coverage (Code Section 6055).
Determine which reporting requirements apply to you and your health plans
Determine the information you will need for reporting and coordinate internal and external resources to help compile the required data for the 1094-C and 1095-C
Complete the appropriate forms for the 2020 reporting year. Furnish statements to individuals on or before January 31, 2021 has been extended to March 2, 2021 IRS Notice 2020-76., and file returns with the IRS on or before February 28, 2020 (March 31, 2020, if filing electronically).
ACA Requirement
Deadline
1095 forms delivered to employees
Jan. 31 (extended to March 2)
Paper filing with IRS*
Feb. 28
Electronic filing with IRS
March 31
Comparative Effectiveness Research Fee (PCORI)
Sponsors of self-funded plans and health insurance issuers of fully insured plans are required to pay a fee each year, by July 31st, to fund comparative effectiveness research. Fees will increase to $2.45 per covered life in 2020 and are next due July 31, 2021.
W-2 Reporting
Healthcare Reform requires employers to report the aggregate cost of employer-sponsored group health plan coverage on their employees’ Forms W-2. This reporting requirement was originally effective for the 2011 tax year. However, the IRS later made reporting optional for 2011 for all employers.
The IRS further delayed the reporting requirement for small employers (those that file fewer than 250 Forms W-2) by making it optional for these employers until further guidance is issued. For the larger employers, the reporting requirement was mandatory for the 2012 Forms W-2 and continues.
ACA DISCLOSURE REQUIREMENTS
Summary of Benefits and Coverage
The ACA requires health plans and health insurance issuers to provide an SBC to applicants and enrollees to help them understand their coverage and make coverage decisions. Plans and issuers must provide the SBC to participants and beneficiaries who enroll or re-enroll during an open enrollment period. The SBC also must be provided to participants and beneficiaries who enroll other than through an open enrollment period (including those who are newly eligible for coverage and special enrollees).
In connection with a plan’s 2020 open enrollment period, the SBC should be included with the plan’s application materials. If coverage automatically renews for current participants, the SBC must generally be provided no later than 30 days before the beginning of the new plan year.
For self-funded plans, the plan administrator is responsible for providing the SBC. For insured plans, both the plan and the issuer are obligated to provide the SBC, although this obligation is satisfied for both parties if either one provides the SBC. Thus, if you have an insured plan, you should confirm that your health insurance issuer will assume responsibility for providing the SBCs.
Grandfathered Plan Notice
If you have a grandfathered plan, make sure to include information about the plan’s grandfathered status in plan materials describing the coverage under the plan, such as SPDs and open enrollment materials. Model language is available from the DOL.
Notice of Patient Protections
Under the ACA, non-grandfathered group health plans and issuers that require designation of a participating primary care provider must permit each participant, beneficiary and enrollee to designate any available participating primary care provider (including a pediatrician for children). Also, plans and issuers that provide obstetrical/gynecological care and require a designation of a participating primary care provider may not require preauthorization or referral for obstetrical/gynecological care.
If a non-grandfathered plan requires participants to designate a participating primary care provider, the plan or issuer must provide a notice of these patient protections whenever the SPD or similar description of benefits is provided to a participant. If your plan is subject to this notice requirement, you should confirm that it is included in the plan’s open enrollment materials. Model language is available from the DOL.
OTHER NOTICES
Group health plan sponsors should consider including the following enrollment and annual notices with the plan’s open enrollment materials.
Initial COBRA Notice
The Consolidated Omnibus Budget Reconciliation Act (COBRA) applies to employers with 20 or more employees that sponsor group health plans. Plan administrators must provide an initial COBRA notice to new participants and certain dependents within 90 days after plan coverage begins. The initial COBRA notice may be incorporated into the plan’s SPD. A model initial COBRA notice is available from the DOL.
Notice of HIPAA Special Enrollment Rights
At or prior to the time of enrollment, a group health plan must provide each eligible employee with a notice of his or her special enrollment rights under HIPAA. This notice may be included in the plan’s SPD. Model language for this disclosure is available on the DOL’s website.
Annual CHIPRA Notice
Group health plans covering residents in a state that provides a premium subsidy to low-income children and their families to help pay for employer-sponsored coverage must send an annual notice about the available assistance to all employees residing in that state. The DOL has provided a model notice.
WHCRA Notice
Plans and issuers must provide notice of participants’ rights to mastectomy-related benefits under the Women’s Health and Cancer Rights Act (WHCRA) at the time of enrollment and on an annual basis. Model language for this disclosure is available on the DOL’s website.
NMHPA Notice
Plan administrators must include a statement within the Summary Plan Description (SPD) timeframe describing requirements relating to any hospital length of stay in connection with childbirth for a mother or newborn child under the Newborns’ and Mothers’ Health Protections Act. Model language for this disclosure is available on the DOL’s website.
Medicare Part D Notices
Group health plan sponsors must provide a notice of creditable or non-creditable prescription drug coverage to Medicare Part D eligible individuals who are covered by, or who apply for, prescription drug coverage under the health plan. This creditable coverage notice alerts the individuals as to whether or not their prescription drug coverage is at least as good as the Medicare Part D coverage. The notice generally must be provided at various times, including when an individual enrolls in the plan and each year before Oct. 15th(when the Medicare annual open enrollment period begins). Model notices are available on the Centers for Medicare and Medicaid Services’ website.
HIPAA Privacy Notice
The HIPAA Privacy Rule requires covered entities (including group health plans and issuers) to provide a Notice of Privacy Practices (or Privacy Notice) to each individual who is the subject of protected health information (PHI). Health plans are required to send the Privacy Notice at certain times, including to new enrollees at the time of enrollment. Also, at least once every three years, health plans must either redistribute the Privacy Notice or notify participants that the Privacy Notice is available and explain how to obtain a copy.
Self-insured health plans are required to maintain and provide their own Privacy Notices. Special rules, however, apply for fully insured plans. Under these rules, the health insurance issuer, and not the health plan itself, is primarily responsible for the Privacy Notice.
Model Privacy Notices are available through the Department of Health and Human Services
Summary Plan Description (SPD)
Plan administrators must provide an SPD to new participants within 90 days after plan coverage begins. Any changes that are made to the plan should be reflected in an updated SPD booklet or described to participants through a summary of material modifications (SMM).
Also, an updated SPD must be furnished every five years if changes are made to SPD information or the plan is amended. Otherwise, a new SPD must be provided every 10 years.
Summary Annual Report
Plan administrators that are required to file a Form 5500 (> 100 participants in plan) must provide participants with a narrative summary of the information in the Form 5500, called a summary annual report (SAR). The plan administrator generally must provide the SAR within nine months of the close of the plan year. If an extension of time to file the Form 5500 is obtained, the plan administrator must furnish the SAR within two months after the close of the extension period.
Wellness Program Notices
Group health plans that include wellness programs may be required to provide certain notices regarding the program’s design. As a general rule, these notices should be provided when the wellness program is communicated to employees and before employees provide any health-related information or undergo medical examinations.
HIPAA Wellness Program Notice—HIPAA imposes a notice requirement on health-contingent wellness programs that are offered under group health plans. Health-contingent wellness plans require individuals to satisfy standards related to health factors (for example, not smoking) in order to obtain rewards. The notice must disclose the availability of a reasonable alternative standard to qualify for the reward (and, if applicable, the possibility of waiver of the otherwise applicable standard) in all plan materials describing the terms of a health-contingent wellness program. Final regulations provide sample language that can be used to satisfy this requirement.
ADA Wellness Program Notice—Employers with 15 or more employees are subject to the Americans with Disabilities Act (ADA). Wellness programs that include health-related questions or medical examinations must comply with the ADA’s requirements, including an employee notice requirement. Employers must give participating employees a notice that tells them what information will be collected as part of the wellness program, with whom it will be shared and for what purpose, the limits on disclosure and the way information will be kept confidential. The Equal Employment Opportunity Commission (EEOC) has provided a sample notice to help employers comply with this ADA requirement.
Enhance Your Employee Benefits Package. A competitive benefits package is key to keeping and attracting top talent.Assess your current benefits package and consider making necessary adjustments to include options, such as expanded mental health support, for example.
GENERAL HR
Review Employee Records. The fourth quarter is a good time to review your employee records and check record retention guidelines. Don’t forget to dispose of outdated termination and outdated job applications properly. With W2s around the corner, make sure all addresses and information are updated.
Develop and Distribute Your 2022 Calendar. Create and distribute a calendar outlining important dates, vacation time, pay dates, and company-observed holidays for 2022.
Review and Update Employee Handbook. Review your employee handbook to make sure it is up-to-date and addresses areas, such as employment law mandates, new COVID-related policies, guidelines for remote working, privacy policies, compensation and performance reviews, social media policies, attendance, and time-off, break periods, benefits, and procedures for termination, discipline, workplace safety, and emergency procedures.
PLEASE NOTE: This information is for general reference purposes only. Because laws, regulations, and filing deadlines are likely to change, please check with the appropriate organizations or government agencies for the latest information and consult your employment attorney and/or benefits advisor regarding your responsibilities. In addition, your business may be exempt from certain requirements and/or be subject to different requirements under the laws of your state. (Updated Oct. 3, 2021)
Contact us at (855) 667-4621 or email us at info@medicalsolutionscorp.com
Employee Retention Tax Credits under CARES ACT have been available yet there has been confusion surrounding this. Employee Retention Tax Credits (ERTC). Much of this has been covered under Corona Virus Resource Page –What the Coronavirus Means for Your Business. The ERTC was extended and modified by the Consolidated Appropriations Act of 2021.
COVID-19 Employee Retention Credit available for Businesses Financially Impacted
The Treasury Department and the Internal Revenue Service today launched the Employee Retention Credit, designed to encourage businesses to keep employees on their payroll. The refundable tax credit is 50% of up to $10,000 in wages paid by an eligible employer whose business has been financially impacted by COVID-19.
FAQ
Does my business qualify to receive the Employee Retention Credit?
The credit is available to all employers regardless of size, including tax-exempt organizations. There are only two exceptions: State and local governments and their instrumentalities and small businesses who take small business loans.
Qualifying employers must fall into one of two categories:
1.The employer’s business is fully or partially suspended by government order due to COVID-19 during the calendar quarter.
2. The employer’s gross receipts are below 50% of the comparable quarter in 2019. Once the employer’s gross receipts go above 80% of a comparable quarter in 2019, they no longer qualify after the end of that quarter.
How is the credit calculated?
The amount of the credit is 50% of qualifying wages paid up to $10,000 in total. Wages paid after March 12, 2020, and before Jan. 1, 2021, areeligible for the credit. Wages taken into account are not limited to cash payments, but also include a portion of the cost of employer-providedhealth care.
How do I know which wages qualify?
Qualifying wages are based on the average number of a business’s employees in 2019.Employers with less than 100 employees: If the employer had 100 or fewer employees on average in 2019, the credit is based on wages paid toall employees, regardless if they worked or not. If the employees worked full time and were paid for full-time work, the employer still receivesthe credit.
Employers with more than 100 employees: If the employer had more than 100 employees on average in 2019, then the credit is allowed only forwages paid to employees who did not work during the calendar quarter.
I am an eligible employer. How do I receive my credit?
Employers can be immediately reimbursed for the credit by reducing their required deposits of payroll taxes that have been withheld fromemployees’ wages by the amount of the credit.
Eligible employers will report their total qualified wages and the related health insurance costs for each quarter on their quarterly employmenttax returns or Form 941 beginning with the second quarter. If the employer’s employment tax deposits are not sufficient to cover the credit, theemployer may receive an advance payment from the IRS by submitting Form 7200, Advance Payment of Employer Credits Due to COVID-19.
Eligible employers can also request an advance of the Employee Retention Credit by submitting Form 7200.
Where can I find more information on the Employer Retention Credit and other COVID-19 economic relief efforts?
Updates on the implementation of this Employee Retention Credit, Frequently Asked Questions on Tax Credits for Required Paid Leave andother information can be found on the Coronavirus page ofIRS.gov.
Do you have a Checklist for the Paycheck Protection Loans Documentations?
Start preparing NOW. Gather documents that provide proof of payment for allowable expenses under the Paycheck Protection Program and be ready to make related certifications for the application.
I’m working with a PEO, how do I get these forms to the IRS?
When partnering with a PEO, the PEO mayrequest an attestation from the client or theclient‘s CPA certifying that the client qualifies for the ERTC.This is because the PEO is unable to verify that the client incurred a reduction in gross receipts or otherwise qualified for the credit.Furthermore, indemnification may be requested, given that incongruities with claiming the credit mustbe reconciled on the PEO‘s Form 941.Finally,in order to prevent multiple filings, it is possible that a PEO may establish deadlines for clients claiming the ERTC and impose an administrative fee associated with processing the ERTC for former clients or clients seeking to claim the credit outside of specifiedtime frames.
For more information about the ERTC, please contact your PEO service provider.
The IRS has released the 2022 Health Savings Account (HSA) inflation adjustments. To be eligible to make HSA contributions, an individual must be covered under a high deductible health plan (HDHP) and meet certain other eligibility requirements.
New HSA 2022 limits are as follows:
2022
2021
HSA Annual Contribution Limit
$3,650; $7,300
$3,600 – Single; $7,200 – Family
HDHP Minimum Annual Deductible
$1,400; $2,800
$1,400 – Single; $2,800 – Family
HDHP Out-of-Pocket Maximum
$7,050; $14,100
$7,000 – Single; $14,000 – Family
Age 55+ Catch-Up Provision
$1,000; $2,000
$1,000- Single; $2,000 – H/W
Age 55 Catch Up Contribution
As in 401k and IRA contributions, you are allowed to contribute extra if you are above a certain age. If you are age 55 or older by the end of the year, you can contribute an additional $1,000 to your HSA. If you are married, and both of you are age 55, each of you can contribute an additional $1,000. A savvy strategy for high-income earners is to invest the money in your HSA for the long haul. Once you’re 65, you can take out tax-free distributions to cover Medicare premiums. If you withdraw money at that point for non-medical uses, you pay the same tax as you would on withdrawals from a pretax 401(k). But you can also take money out tax-free to reimburse yourself for prior years’ out-of-pocket medical expenses if you have the old receipts.
COVId-19 Update:
You can even use an HSA to save on a typical trip to the CVS. Thanks to a tax relief provision tucked in the last Covid-19 stimulus package, you can use the money you stash in an HSA or FSA (more on those later) for over-the-counter medications like Tylenol or Flonase as well as menstrual products like tampons and pads. That reverses Obamacare restrictions on OTC meds requiring a doctor’s prescription for them to be eligible for reimbursement.
HSA/HDHP Market Growth
HSA holders own the assets in the accounts and can build up substantial sums over time. Enrollment in HSA-compatible insurance plans has increased to 10 million earlier this year, from 1 million in March 2005, according to, America’s Health Insurance Plans (AHIP), a trade group.
HSAs were authorized starting in January 2004. Since then, AHIP has conducted a periodic census of health plans participating in the HSA/HDHP market.
The number of people with HSA/HDHP coverage rose to more than 11.4 in January 2011, up from 10.0 million in January 2010, 8.0 million in January 2009, and 6.1 million in January 2008.
30 percent of individuals covered by an HSA plan were in the small group market, 50 percent were in the large-group market, and the remaining 20 percent were in the individual market.
14% of all workers in the private sector have access to a Health Savings Account acc. to the Bureau of Labor Statistics.
States with the highest levels of HSA/HDHP enrollment were California, Ohio, Florida, Texas, Illinois, and Minnesota.
HSA Advantages:
Opportunity to build savings – Unused money stays in your account from year to year and earns tax-free interest. The HSA also gives you an investment opportunity.
Tax-free contributions and earnings – You don’t pay taxes on contributions or earnings.
Tax-Free Money allowed for non-traditional Medical coverage– As per IRS Publication 502, unused money can be used for dental, vision, Lasik eye surgery, acupuncture, yoga, infertility, etc. Popular Examples
Portability – The funds belong to you, so you keep the funds if you change jobs or retire.
Our overall experience with HSAs has been positive when employer funding is at a minimum 50% using either the HSA or an HRA (Health Reimbursement Account-employer keeps unspent money). Traditional plans trend of higher copays and new in-network deductibles has also led to the popularity of an HSA.
Next Steps
Plan sponsors should update payroll and plan administration systems for the 2022 cost-of-living adjustments and should incorporate the new limits in relevant participant communications, such as open enrollment and communication materials, plan documents, and summary plan descriptions.
Is your HSA compliant? Which pre-tax qualified HSA, FSA, HRA spending card is right for you? Please contact our team at Millennium Medical Solutions Corp (855)667-4621 for immediate answers. Stay tuned for updates as more information gets released. Sign up for the latest news updates.
PEO White Papers: The PEO Industry Footprint in 2021
Professional employer organizations (PEOs) provide comprehensive HR solutions for small and mid-sized businesses by supplying them with a broad array of cost-effective HR offerings and expertise. This enables PEO clients to concentrate on growing their businesses while offering superior benefits and HR practices to their employees. Research in our previous white papers has shown multiple positive effects from these services: PEO clients enjoy a better chance of survival, higher growth rates, lower employee turnover, higher employee satisfaction, and they fared better during the COVID-19 pandemic.
KEY FINDINGS:
NAPEO’s White Paper series aims to help the general public and small business owners better understand the economic impact and value of the PEO industry and the ways working with a PEO can help businesses grow and thrive.
Our white papers have shown that:
Businesses in a PEO arrangement grow 7-9 percent faster, have 10-14 percent lower turnover, and are 50 percent less likely to go out of business.
Click Above
PEOs are able to offer a broad array of HR services at a lower cost and offer access to retirement plans to small businesses that may not otherwise sponsor them.
PEOs provide services to 175,000 small and mid-sized businesses, employing 3.7 million people.
There are 907 PEOs in the United States.
The total employment represented by the PEO industry is roughly the same as the combined number of employees for Walmart (United States only), Amazon, IBM, FedEx, Starbucks, AT&T, Wells Fargo, Apple, and Google.
The PEO industry’s 175,000 clients represent 15 percent of all employers with 10 to 99 employees.
Administrative costs are around $450 lower per employee for businesses that use a PEO.
PPE Expenses May Be Reimbursable Under Health Spending Accounts – Video
During the COVID-19 pandemic, you may have purchased masks or PPE for the purpose of preventing the spread of the COVID-19. Now, according to a recent announcement from the IRS, those purchases may be deductible from your income for tax purposes and eligible to be paid or reimbursed under certain savings accounts. This video explains further:
If you’re interested in hearing more about the advantages of partnering with a PEO, we’d love to talk to you. Fill out the form below or email info@medicalsolutionscorp.com for a FREE Consultation Today!
The information provided on this website is intended for informational purposes only. Millennium Medical Solutions Corp. does not offer legal or medical guidance. Those with legal or medical questions should seek appropriate assistance from a licensed professional. Stay up to date by signing up for Newsletter and Coronavirus Dashboard below.
When choosing the right PEO, especially when it comes to human resource management, you should ensure that they offer basic HR services like benefits, payroll, and compliance.
Pros of PEO
1. Flexible, scalable:
Bundled HR solution covers you as you grow.i.e. Compliance changes based on # of employees. The HR Platform can handle 10 as well as 200 employees. The benefits scale up as you do. You are able to include value-added services as you grow.
2. Access to “Big-Company” infrastructure and benefits
More health care benefit options for employees and their families mean:
Attract high caliber talent in your industry
Retain your best employees
401(k) and retirement planning
Top-rated voluntary benefits and discount programs
HR technology platform for administering benefit plans
3. Access to HR expertise
Support for payroll and employee needs.
HR and Human Capital consultants.
Benefits administration
Employee issues
Strategic HR planning: Interview Traning and Permanence Management Reviews, etc.
Ensure HR compliance with local, state and federal laws.
4. Shifting and sharing of liability
Workplace safety
Sexual Harassment
Employer Practices Liability Insurance
Affordable Care Act compliance
COVID and New regulations
5. Value
Time Saver: You get back valuable time from doing redundancies. The average PEO client saves 10 hrs/month.
Benefits Savings: The average client saves 15-40% on medical benefits alone. The national networks and robust benefits are also value-added.
Savings on Workmans Comp.
PEO’s are pay as you go WC. This means if you downsized in light of COVID you receive an adjusted lower rate the following month and not end of the year.
PEO’s may be able to place hard to write Workmans Comp. Ex: Construction Industry
State Unemployment: Since you are sharing in a larger company’s SUTA rate the rates are generally lower with lower fluctuations. If during COVID a company had high turnover their SUTA rate can jump much higher than a PEO.
PEO Cons
1. Wrong PEO Selecting a PEO for the wrong reason(s): should be considered a long-term strategy, not a short-term fix. Some PEOs may charge a percentage of salary instead of a clear per employee per month cost.
2. Employers fear the loss of control Even though you will still be running your small business and making day to day decisions, the PEO will become the co-employer of your staff. PEOs do NOT have control over your salary. You control who you hire/fire. You decide on benefits eligibility waiting periods, plan selections, and employer contributions. The PEOs deal with HR responsibilities and risks, saving you countless hours and many headaches, but do not take away your independence.
3 System limitations Because the PEO is a business as well, and has to meet it’s own deadlines, they may request certain payments upfront. This may mean a fundamental shift in your cash flow because there will be consequences for being a week late with your payroll taxes.
4. It is NOT for every small business depending on your industry and demographics you may or may not be the right for a PEO. While the vast majority of clients are indeed enjoying benefits savings for some groups the costs may be even higher than small group health insurance. Addiotnaly, some companies can develop above-average very high risk and become too much of a liability burden for the PEO and the client can be moved to a higher risk category. The very advantage of a PEO can make it a disadvantage – they can underwrite.
Summary
Before you consider hiring a Professional Employment Organization, you should first find out what is a PEO so that you can know exactly what to expect from it. With the right PEO, you will be able to manage your businesses’ demand for growth and your employees as well.
If you are looking for an insurance solution for your business, go to our website and check out our business insurance solutions. Do not hesitate tocontact usfor more information.
A little-known requirement but most important under Affordable Care Act (ACA) is for Health Insurers must waive their minimum employer-contribution and employee-participation rules once a year. ACA requires a one-month Special Open Enrollment Window for January 1st coverage.
The special open enrollment period occurs November 15th through December 15th of each year, allowing eligible small group employers to enroll for coverage effective January 1st of the following year.
Background
The ACA has a section in it called the “guaranteed issuance of coverage in the individual and group market.” It stipulates that “each health insurer that offers health insurance coverage in the individual or group market in the state must accept every employer and individual in the state that applies for such coverage.” The section also states that this guaranteed issuance of coverage can only be offered during (special) open enrollment periods, and that plans can only be offered to applicants that live in, work in, or reside in the plans’ service area(s).
Participation and Contribution Requirements
In many states (including California and Nevada), carriers can decline to issue group health coverage if fewer than 70% of employees elect to enroll in coverage. Some carriers may have even tighter participation requirements.
Generally speaking, employees with other coverage (Medicare, other group coverage, individual coverage through the Exchange, etc.) are removed from the participation requirement calculation – though it varies by insurance carrier.
Furthermore, employer contribution rules require employers to contribute a certain percentage of premium costs for all employees in order to attain group health coverage. Some businesses struggle to meet these contribution requirements for a variety of financial reasons.
Problem Solved: Special Open Enrollment Period
Many employers want to offer coverage to their employees, but are denied because they struggle to meet participation and/or contribution requirements. Employers cannot force employees to enroll in coverage unless the employer pays for 100% of the employees’ premiums, which many employers cannot afford. Even with moderate to generous employer contributions, many employers still find young and lower-income employees waiving coverage. This was even more evident in 2019 with the ACA’s federal Individual Mandate non-compliance penalty reduced to $0.00.
The U.S. Department of Health & Human Services provides final guidance on this in regulation 147.104(b)(1): “In the case of health insurance coverage offered in the small group market, a health insurance issuer may limit the availability of coverage to an annual enrollment period that begins November 15 and extends through December 15 of each year in the case of a plan sponsor that is unable to comply with a material plan provision relating to employer contribution or group participation rules.”
If your employer groups are struggling with participation and/or contribution, the Special Open Enrollment Window is the time to enroll them in coverage.
This Compliance Overview is not intended to be exhaustive nor should any discussion or opinions be construed as legal advice. Readers should contact legal counsel for legal advice.
In preparation for open enrollment, Employers should review their plan documents in light of changes for the plan year beginning Jan 1, 2021. Below is an Employer 2 Open Enrollment Checklist including some administrative items to prepare for in 2020.
Health plan sponsors should also confirm that their open enrollment materials contain certain required participant notices, when applicable—for example, the summary of benefits and coverage (SBC). There are also some participant notices that must be provided annually or upon initial enrollment. To minimize costs and streamline administration, employers should consider including these notices in their open enrollment materials.
PLAN DESIGN CHANGES
Out-of-pocket Maximum
Effective for plan years beginning on or after Jan. 1, 2014, non-grandfathered health plans are subject to limits on cost-sharing for essential health benefits (EHB). The ACA’s out-of-pocket maximum applies to all non-grandfathered group health plans, including self-insured health plans and insured plans.
$8,550 for self-only coverage and $17,100 for family coverage out-of-pocket maximum.
$7,000 for self-only coverage and $14,000 for family coverage HSA Maximum. For 2021 plan years, the out-of-pocket maximum limit for HDHPs is $7,000 for self-only coverage and $14,000 for family coverage.
Preventive Care Benefits
The ACA requires non-grandfathered health plans to cover certain preventive health services without imposing cost-sharing requirements (that is, deductibles, copayments or coinsurance) for the services. Health plans are required to adjust their first-dollar coverage of preventive care services based on the latest preventive care recommendations. If you have a non-grandfathered plan, you should confirm that your plan covers the latest recommended preventive care services without imposing any cost-sharing.
The ACA imposes a dollar limit on employees’ salary reduction contributions to a health flexible spending account (FSA) offered under a cafeteria plan. An employer may impose its own dollar limit on employees’ salary reduction contributions to a health FSA, as long as the employer’s limit does not exceed the ACA’s maximum limit in effect for the plan year.
The ACA set the health FSA contribution limit at $2,500. For years after 2013, the dollar limit is indexed for cost-of-living adjustments. For 2021 plan years, the health FSA limit is $2,750.
Communicate the health FSA limit to employees as part of the open enrollment process.
HDHP and HSA Limits for 2021
If you offer an HDHP to your employees that is compatible with an HSA, you should confirm that the HDHP’s minimum deductible and out-of-pocket maximum comply with the 2020 limits. The IRS limits for HSA contributions and HDHP cost-sharing increase for 2020. The HSA contribution limits will increase effective Jan. 1, 2020, while the HDHP limits will increase effective for plan years beginning on or after Jan. 1, 2020.
Check whether your HDHP’s cost-sharing limits need to be adjusted for the 2020 limits.
If you communicate the HSA contribution limits to employees as part of the enrollment process, these enrollment materials should be updated to reflect the increased limits that apply for 2020.
The following table contains the HDHP and HSA limits for 2020 as compared to 2019. It also includes the catch-up contribution limit that applies to HSA-eligible individuals who are age 55 or older, which is not adjusted for inflation and stays the same from year to year.
Type of Limit
2020
2021
Change
HSA Contribution Limit
Self-only
$3,500
$3,600
Up $50
Family
$7,100
$7,200
Up $100
HSA Catch-up Contributions (not subject to adjustment for inflation)
Age 55 or older
$1,000
$1,000
No change
HDHP Minimum Deductible
Self-only
$1,400
$1,400
No change
Family
$2,800
$2,800
No change
HDHP Maximum Out-of-pocket Expense Limit (deductibles, copayments and other amounts, but not premiums)
Self-only
$6,900
$7,000
Up $100
Family
$13,800
$14,000
Up $200
ACA EMPLOYER MANDATE AND OTHER REQUIREMENTS
Applicable Large Employer Status (ALE)
Under the ACA’s employer penalty rules, applicable large employers (ALEs) that do not offer health coverage to their full-time employees (and dependent children) that is affordable and provides minimum value will be subject to penalties if any full-time employee receives a government subsidy for health coverage through an Exchange.
To qualify as an ALE, an employer must employ, on average, at least 50 full-time employees, including full-time equivalent employees (FTEs), on business days during the preceding calendar year. All employers that employ at least 50 full-time employees, including FTEs, are subject to the ACA’s pay or play rules.
Determine your ALE status for 2021
Calculate the number of full-time employees for all 12 calendar months of 2020. A full-time employee is an employee who is employed on average for at least 30 hours of service per week.
Calculate the number of FTEs for all 12 calendar months of 2020 by calculating the aggregate number of hours of service (but not more than 120 hours of service for any employee) for all employees who were not full-time employees for that month and dividing the total hours of service by 120.
Add the number of full-time employees and FTEs (including fractions) calculated above for all 12 calendar months of 2020.
Add up the monthly numbers from the preceding step and divide the sum by 12. Disregard fractions.
If your result is 50 or more, you are likely an ALE for 2021.
Identify Full-time Employees
All full-time employees must be offered affordable minimum value coverage. A full-time employee is an employee who was employed on average at least 30 hours of service per week. The final regulations generally treat 130 hours of service in a calendar month as the monthly equivalent of 30 hours of service per week. The IRS has provided two methods for determining full-time employee status—the monthly measurement method and the look-back measurement method.
Determine which method you are going to use to determine full-time status
Monthly measurement method involves a month-to-month analysis where full-time employees are identified based on their hours of service for each month. This method is not based on averaging hours of service over a prior measurement method. Month-to-month measuring may cause practical difficulties for employers, particularly if there are employees with varying hours or employment schedules, and could result in employees moving in and out of employer coverage on a monthly
Look-back measurement method allows an employer to determine full-time status based on average hours worked by an employee in a prior period. This method involves a measurement period for counting/averaging hours of service, an administrative period that allows time for enrollment and disenrollment, and a stability period when coverage may need to be provided, depending on an employee’s average hours of service during the measurement
Offer of Coverage
An ALE may be liable for a penalty under the pay or play rules if it does not offer coverage to “substantially all” (95%) full-time employees (and dependents) and any one of its full-time employees receives a premium tax credit or cost-sharing reduction for coverage purchased through an Exchange. Employees who are offered health coverage that is affordable and provides minimum value are generally not eligible for these Exchange subsidies.
Offer minimum essential coverage to all full-time employees
Ensure that at least one of those plans provides minimum value (60% actuarial value)
Ensure that the minimum value plan offered is affordable to all full-time employees by ensuring that the employee contribution for the lowest cost single minimum value plan does not exceed 78% of an employee’s earnings based on the employee’s W-2 wages, the employee’s rate of pay, or the federal poverty level for a single individual.
Reporting of Coverage
The ACA requires ALEs to report information to the IRS and to employees regarding the employer-sponsored health coverage on Form 1095-C. The IRS will use the information that ALEs report to verify employer-sponsored coverage and to administer the employer shared responsibility provisions (Code Section 6056).
In addition, the ACA requires every health insurance issuer, sponsor of a self-insured health plan, a government agency that administers government-sponsored health insurance programs and any other entity that provides minimum essential coverage (MEC) to file an annual return with the IRS and individuals reporting information for each individual who is provided with this coverage (Code Section 6055).
Determine which reporting requirements apply to you and your health plans
Determine the information you will need for reporting and coordinate internal and external resources to help compile the required data for the 1094-C and 1095-C
Complete the appropriate forms for the 2020 reporting year. Furnish statements to individuals on or before January 31, 2021 has been extended to March 2, 2021 IRS Notice 2020-76., and file returns with the IRS on or before February 28, 2020 (March 31, 2020, if filing electronically).
ACA Requirement
Deadline
1095 forms delivered to employees
Jan. 31 (extended to March 2)
Paper filing with IRS*
Feb. 28
Electronic filing with IRS
March 31
Comparative Effectiveness Research Fee (PCORI)
Sponsors of self-funded plans and health insurance issuers of fully insured plans are required to pay a fee each year, by July 31st, to fund comparative effectiveness research. Fees will increase to $2.45 per covered life in 2020 and are next due July 31, 2021.
W-2 Reporting
Healthcare Reform requires employers to report the aggregate cost of employer-sponsored group health plan coverage on their employees’ Forms W-2. This reporting requirement was originally effective for the 2011 tax year. However, the IRS later made reporting optional for 2011 for all employers.
The IRS further delayed the reporting requirement for small employers (those that file fewer than 250 Forms W-2) by making it optional for these employers until further guidance is issued. For the larger employers, the reporting requirement was mandatory for the 2012 Forms W-2 and continues.
ACA DISCLOSURE REQUIREMENTS
Summary of Benefits and Coverage
The ACA requires health plans and health insurance issuers to provide an SBC to applicants and enrollees to help them understand their coverage and make coverage decisions. Plans and issuers must provide the SBC to participants and beneficiaries who enroll or re-enroll during an open enrollment period. The SBC also must be provided to participants and beneficiaries who enroll other than through an open enrollment period (including those who are newly eligible for coverage and special enrollees).
In connection with a plan’s 2020 open enrollment period, the SBC should be included with the plan’s application materials. If coverage automatically renews for current participants, the SBC must generally be provided no later than 30 days before the beginning of the new plan year.
For self-funded plans, the plan administrator is responsible for providing the SBC. For insured plans, both the plan and the issuer are obligated to provide the SBC, although this obligation is satisfied for both parties if either one provides the SBC. Thus, if you have an insured plan, you should confirm that your health insurance issuer will assume responsibility for providing the SBCs.
Grandfathered Plan Notice
If you have a grandfathered plan, make sure to include information about the plan’s grandfathered status in plan materials describing the coverage under the plan, such as SPDs and open enrollment materials. Model language is available from the DOL.
Notice of Patient Protections
Under the ACA, non-grandfathered group health plans and issuers that require designation of a participating primary care provider must permit each participant, beneficiary and enrollee to designate any available participating primary care provider (including a pediatrician for children). Also, plans and issuers that provide obstetrical/gynecological care and require a designation of a participating primary care provider may not require preauthorization or referral for obstetrical/gynecological care.
If a non-grandfathered plan requires participants to designate a participating primary care provider, the plan or issuer must provide a notice of these patient protections whenever the SPD or similar description of benefits is provided to a participant. If your plan is subject to this notice requirement, you should confirm that it is included in the plan’s open enrollment materials. Model language is available from the DOL.
OTHER NOTICES
Group health plan sponsors should consider including the following enrollment and annual notices with the plan’s open enrollment materials.
Initial COBRA Notice
The Consolidated Omnibus Budget Reconciliation Act (COBRA) applies to employers with 20 or more employees that sponsor group health plans. Plan administrators must provide an initial COBRA notice to new participants and certain dependents within 90 days after plan coverage begins. The initial COBRA notice may be incorporated into the plan’s SPD. A model initial COBRA notice is available from the DOL.
Notice of HIPAA Special Enrollment Rights
At or prior to the time of enrollment, a group health plan must provide each eligible employee with a notice of his or her special enrollment rights under HIPAA. This notice may be included in the plan’s SPD. Model language for this disclosure is available on the DOL’s website.
Annual CHIPRA Notice
Group health plans covering residents in a state that provides a premium subsidy to low-income children and their families to help pay for employer-sponsored coverage must send an annual notice about the available assistance to all employees residing in that state. The DOL has provided a model notice.
WHCRA Notice
Plans and issuers must provide notice of participants’ rights to mastectomy-related benefits under the Women’s Health and Cancer Rights Act (WHCRA) at the time of enrollment and on an annual basis. Model language for this disclosure is available on the DOL’s website.
NMHPA Notice
Plan administrators must include a statement within the Summary Plan Description (SPD) timeframe describing requirements relating to any hospital length of stay in connection with childbirth for a mother or newborn child under the Newborns’ and Mothers’ Health Protections Act. Model language for this disclosure is available on the DOL’s website.
Medicare Part D Notices
Group health plan sponsors must provide a notice of creditable or non-creditable prescription drug coverage to Medicare Part D eligible individuals who are covered by, or who apply for, prescription drug coverage under the health plan. This creditable coverage notice alerts the individuals as to whether or not their prescription drug coverage is at least as good as the Medicare Part D coverage. The notice generally must be provided at various times, including when an individual enrolls in the plan and each year before Oct. 15th(when the Medicare annual open enrollment period begins). Model notices are available on the Centers for Medicare and Medicaid Services’ website.
HIPAA Privacy Notice
The HIPAA Privacy Rule requires covered entities (including group health plans and issuers) to provide a Notice of Privacy Practices (or Privacy Notice) to each individual who is the subject of protected health information (PHI). Health plans are required to send the Privacy Notice at certain times, including to new enrollees at the time of enrollment. Also, at least once every three years, health plans must either redistribute the Privacy Notice or notify participants that the Privacy Notice is available and explain how to obtain a copy.
Self-insured health plans are required to maintain and provide their own Privacy Notices. Special rules, however, apply for fully insured plans. Under these rules, the health insurance issuer, and not the health plan itself, is primarily responsible for the Privacy Notice.
Model Privacy Notices are available through the Department of Health and Human Services
Summary Plan Description (SPD)
Plan administrators must provide an SPD to new participants within 90 days after plan coverage begins. Any changes that are made to the plan should be reflected in an updated SPD booklet or described to participants through a summary of material modifications (SMM).
Also, an updated SPD must be furnished every five years if changes are made to SPD information or the plan is amended. Otherwise, a new SPD must be provided every 10 years.
Summary Annual Report
Plan administrators that are required to file a Form 5500 (> 100 participants in plan) must provide participants with a narrative summary of the information in the Form 5500, called a summary annual report (SAR). The plan administrator generally must provide the SAR within nine months of the close of the plan year. If an extension of time to file the Form 5500 is obtained, the plan administrator must furnish the SAR within two months after the close of the extension period.
Wellness Program Notices
Group health plans that include wellness programs may be required to provide certain notices regarding the program’s design. As a general rule, these notices should be provided when the wellness program is communicated to employees and before employees provide any health-related information or undergo medical examinations.
HIPAA Wellness Program Notice—HIPAA imposes a notice requirement on health-contingent wellness programs that are offered under group health plans. Health-contingent wellness plans require individuals to satisfy standards related to health factors (for example, not smoking) in order to obtain rewards. The notice must disclose the availability of a reasonable alternative standard to qualify for the reward (and, if applicable, the possibility of waiver of the otherwise applicable standard) in all plan materials describing the terms of a health-contingent wellness program. Final regulations provide sample language that can be used to satisfy this requirement.
ADA Wellness Program Notice—Employers with 15 or more employees are subject to the Americans with Disabilities Act (ADA). Wellness programs that include health-related questions or medical examinations must comply with the ADA’s requirements, including an employee notice requirement. Employers must give participating employees a notice that tells them what information will be collected as part of the wellness program, with whom it will be shared and for what purpose, the limits on disclosure and the way information will be kept confidential. The Equal Employment Opportunity Commission (EEOC) has provided a sample notice to help employers comply with this ADA requirement.
Contact us at (855) 667-4621 or email us at info@360PEO.com